Mac Vet Rev 2015; 38 (1): 13 - 20
 10.14432/j.macvetrev.2014.11.026
10.14432/j.macvetrev.2014.11.026
Received: 27 July 2014
Received in revised form: 17 October 2014
Accepted: 01 November 2014
Available Online First: 20 November 2014
Published on: 15 March 2015
Keywords: mitral valve disease, review, dog
When discussing myxomatous valve disease in dogs, one has in mind atrioventricular valves, in particular the mitral valve, which is affected the most commonly and followed by the tricuspid, aortic valve and pulmonic valve, the last being seldom degenerated.
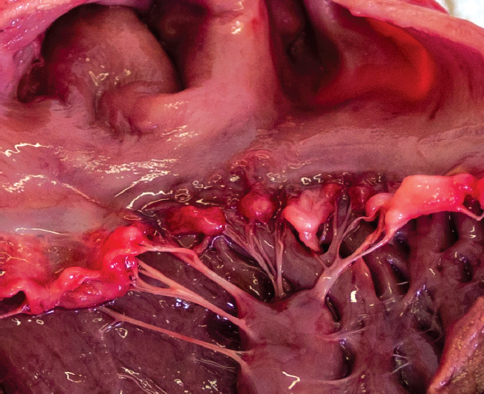
Myxomatous mitral valve disease (MVD) is the most common cause of heart failure in dogs (1). In literature it can be found under various names, such as chronic valve disease, degenerative valve disease, endocardiosis, and chronic myxomatous valvular disease. It is dealt with a chronic degenerative disease with a progressive valve thickening that starts at the valve edges and causes valve insufficiency (Fig. 1). Over time, the degeneration progresses, as does the insufficiency of the valve.
Figure 1 Pathomorphology of the myxomatous mitral valve disease
The disease is typically found in many small-breed dogs, although there are some large breeds that are also predisposed. Breeds such as small mixed breed dogs, Poodles, Yorkshire Terriers, Chihuahuas, Cavalier King Charles Spaniels, Miniature and Standard Schnauzers, Cocker Spaniels, Miniature Pinschers, Pekingese, Shi-Tzu, Dachshunds and Dobermans are most commonly reported (1, 2, 3, 4, 5, 6). Males predominated in most of these studies. Prevalence was strongly associated with breed, age and body size (1, 5).
This disease is very rare in cats, although the actual prevalence in this species is not known.
The disease is characterized by a systolic murmur at the mitral area, which increases in intensity as the disease progresses, and radiates to the right side and to the pulmonary areas. The murmur is a hallmark of the disease and can be found in middle-aged to aged dogs, although Cavalier King Charles Spaniels (CKCS) can be affected as early as from one to two years of age (7). Cavalier King Charles Spaniels seem also to have a higher prevalence of MMVD in comparison to other breeds (8). Murmurs can provide valuable information regarding disease severity; the intensity of the murmur correlates with the severity of MMVD and heart failure class. An increase in the intensity of the S1 sound and a decrease of the S2 sound with the presence of S3 sound are signs of moderate to severe MMVD (9). A right-side murmur can indicate the radiation of a loud mitral murmur to the right side or concomitant tricuspid regurgitation and possible pulmonary hypertension (PHT). A loud systolic right-apical murmur was significantly associated with a tricuspid regurgitant pressure gradient (TR) of ≥ 35 mmHg. A stronger right-than-left apical-murmur had a positive predictive value (PPV) of 83% and was 96% specific for TR≥35 mmHg; when combined with syncope, it had a PPV of 92% and was 92% specific (10). Pedersen’s study revealed that 82% of CKCSs aged one to three years and 97% of dogs aged more than three years had various degrees of mitral valve prolapse, which is one of the predisposition factors for MMVD (7). Other factors that may contribute to the disease are physical, physiological and other types of stress. In addition, endothelial dysfunction further promotes thickening of the valve leaflets due to shear stress (11). Recently, it has been determined that neurotransmitter serotonin concentrations might be associated with MMVD. The study of Ljungvall et al. revealed that dogs with severe MMVD had lower serum serotonin concentrations than healthy dogs (P = .0025) and dogs with mild MMVD (P = .0011). It was found also that serum serotonin concentrations decreased with increasing left-atrial-to-aortic-root ratio (LA/Ao) (12).
In the pathogenesis of the disease, genetic factors play a very important role, which is supported by the fact that the disease is more prevalent in certain breeds of dogs (13).
Direct evidence of genetic influence in MMVD was studied by Swenson in CKCSs and Olsen in Dachshunds (3, 14), although the exact mode of inheritance was not given.
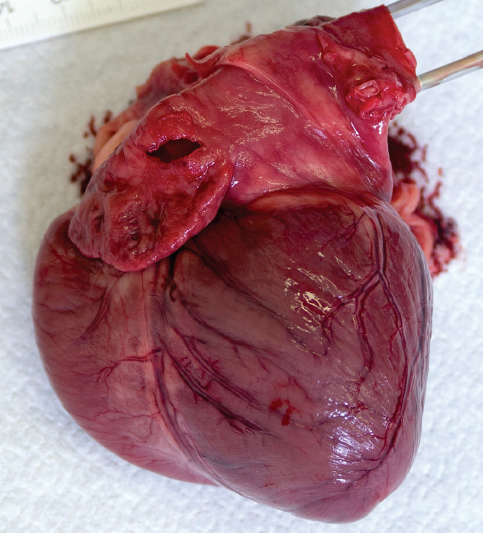
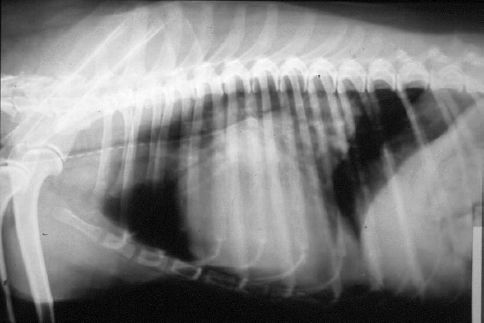
It seems that in dogs that are genetically more burdened the disease progresses more rapidly and at a younger age. The course of the disease can have a few typical courses of progression: 1) It can start at an older age, progress slowly and never end in heart failure; 2) It progresses slowly and then suddenly after chordal rupture progresses rapidly and ends in acute heart failure; 3) It progresses slowly and eventually ends in heart failure; 4) It can progress subclinically and end in sudden death. One reason for sudden death is left atrial rupture, which occurs rarely (Fig. 2). Most commonly, dogs with MMVD die or are euthanized because of progressive heart failure and pulmonary edema (Fig. 3) or worsening of clinical signs (Fig. 4) (4, 5, 15). The majority of dogs with MMVD do not develop congestive heart failure (8) and those dogs have a favorable prognosis, while dogs that develop congestive heart failure have high morbidity. The median survival times of dogs with moderate and severe congestive heart failure (CHF) was 33 and 9 months, respectively (5). Dogs receiving pimobendan instead of benazepril hydrochloride, additionally to diuretics, have significantly longer survival times (16). The quality of life was similar in dogs receiving pimobendan or benazepril, but the time to increase the treatment regime was longer in pimobendan group, heart size was smaller and water retention was less in the pimobendan group (17).
Figure 2 Rupture of the left atrium (LA) between the body of LA and its auricle. A distinct watery sound was heard during systole “in this dog”
Figure 3 Severe cardiogenic pulmonary edema due to MMVD. Mostly left heart enlargement with left atrium elevating trachea at the hilar region. Air bronchograms are evident
Figure 4 Extremely enlarged left atrium elevating and compressing the trachea and causing an almost uncontrollable cough in a 13-year-old Fox Terrier
Dogs with atrial fibrillation had significantly shorter survival (median 195 days) than dogs without this arrhythmia (median survival 632 days) (4). Arrhythmias are seen in dogs in all stages of MMVD; however, supraventricular and other arrhythmias did not appear associated with the level of severity of MMVD (18). Arrhythmias seem to be a rare cause of syncope in MMVD dogs (18). Dogs with a history of syncope and MMVD tend to have decreased heart rate variability (HRV) and sinus arrhythmia compared to dogs without a history of syncope (18).
Despite the fact that this is a disease of the mitral valve, the whole heart undergoes changes that cause its remodeling. The triggering event of these geometrical and structural changes is the increase of end-diastolic pressure and hence end-diastolic wall stress due to the volume overload (19). The leaking valve causes regurgitation of the stroke volume into the low-pressure atrium during systole. The consequence of this wall stress is degradation of the collagen weave between cardiomyocytes. With the progression of mitral valve degeneration, the mitral regurgitation increases, and then the atrio-ventricular annulus dilates and worsens the regurgitant orifice. The LV end-diastolic (EDV) and end-systolic volume (ESV) increase, and the total stroke volume (SV) increase, but the forward stroke volume decreases. The increased wall stress initiates a continuation of collagen loss and myocyte stretch (19). The result is increased end-diastolic LV diameter, and cardiac output is up to 30% less than the baseline output. A recent study revealed that the most cardiac enlargement occurs in the year proceeding congestive heart failure (20).
Increasing end-diastolic volume, increasing wall stress, cardiomyocyte stretch, thinning of the cardiac wall, rounding of the LV apex, and decreased systolic function of the LV despite normal to increased measured shortening fraction (SF%) contribute to the development of the clinical manifestation of the disease.
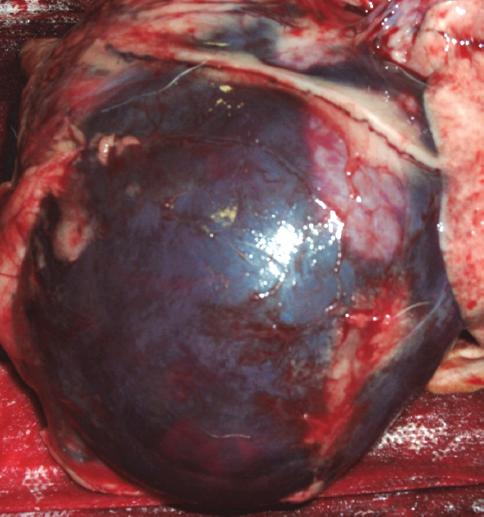
The mitral valve leaflets consist of four distinct layers. The atrial side is called “atriallis” and the ventricular side is called “ventricularis”; both layers consist of endothelial cells. Below these endothelial layers lies a thin layer consisting of collagen fibers, elastic fibers and fibroblasts; on the atrial side there is also smooth muscle. Between the two layers are the spongiosa and the fibrosa layers (19). With the progression of the disease, the endothelium proliferates, and the number of fibroblasts increases; there are areas where the endothelial layer is damaged, exposing the basement membrane or the collagen matrix. The spongiosa proliferates, and the fibrosa degenerates in the course of the disease. The thickened spongiosa has the appearance of mesenchymal tissue, thus, the name “myxomatous” (21). In the spongiosa, myofibroblasts proliferate and form small nodules. In the fibrosa layer, the collagen fibers become swollen and hyalinized, fragmented and vanish. In the region of high velocity, regurgitant jets in the left atrium jet lesions occur and can cause left atrial tear with haemopericard and acute tamponade and/or sudden death (Fig. 5).
Figure 5 Left atrial tear with haemopericard and acute tamponade
As mentioned above, the characteristic systolic plateau-shaped murmur can be heard in the predisposed breeds of dogs, and the disease can have a long asymptomatic course. The symptoms usually begin with the development of left heart failure. The dog is usually presented for tachypnea/dyspnea, cough or syncope. The cough is harsh and dry, can gradually increase in frequency and can be a sign of pulmonary edema or main stem bronchus compression due to enlarged left atrium. A similar cough can also be caused by pulmonary disease such as chronic bronchitis that is common in the small sized dogs and can be mistaken for pulmonary edema. The latter is usually accompanied by tachypnea and/or dyspnea (22). The owner can be asked if the dog has had an increased respiratory rate lately. Normally, the respiratory rate does not exceed 30 breaths per minute in dogs regardless of body weight, age or geographic location (23).
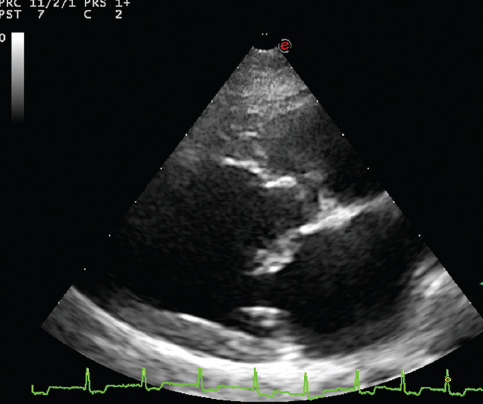
Dyspnea can also be caused by pleural effusion or ascites due to right heart failure. Right heart failure in MMVD is a sign of progressive mitral valve disease and pulmonary hypertension that can be accompanied by tricuspid valve degeneration. Clinical signs may develop gradually and progress or they may come acutely due to sudden worsening of the disease. The owner may not have noticed the gradual declining of the dog’s physical activity, or acute disease may be caused by a rupture of chordae tendinae, the onset of arrhythmia (usually atrial fibrillation) or some kind of stress that puts the animal over the edge (separation from the owner, new environment, exertion). Hearing the typical murmur over the mitral area can determine the diagnosis of MMVD, and heart failure can be confirmed by thoracic radiography (Fig 3). Echocardiography further documents the individual chamber enlargement, the magnitude of regurgitant flow, the severity of mitral degeneration, valve prolapse, chordal rupture and pulmonary hypertension (Fig 6). Systolic function is difficult to assess in MMVD due to the enhanced sympathetic tone (24).
Figure 6 Echocardiographic image showing thickened mitral valve
In an acute setting, which is rare, the cardiac chambers may not be enlarged. In the more common chronic mitral regurgitation, the dilated left ventricular end-diastolic diameter and normal end-systolic diameter, which can also dilate in the late stages of the disease, are usually seen. Therefore, the shortening fraction is increased (over 50%) and comes to normal with advanced disease. Left ventricular end-diastolic diameter, left atrium to aorta ratio (LA/Ao) are echocardiographic measures that independently predict the risk of heart failure (22). The same study confirmed that a radiographically estimated vertebral heart score > 12 and plasma N terminal pro B-type natriuretic peptide (NT pro-BNP) > 1500 pmol/L are measures of threatened heart failure (22).
Electrocardiography serves to identify rhythm disturbances, which are more common in the advanced stages of the disease. The most commonly seen ECG changes are of chamber enlargement, atrial premature complexes, atrial fibrillation, sinus tachycardia, and less commonly ventricular arrhythmias.
Radiographically, stages of left ventricular and left atrial enlargement with more or less or no pulmonary edema (Fig. 4) are perceived as interstitial and alveolar patterns. The latter is seen in severe pulmonary edema.
Treatment options for MMVD
The new treatment recommendations for the MMVD rely on the new ACVIM (American College of Veterinary Internal Medicine) classification of cardiac disease that was adapted from the American College of Cardiology and uses an A-through-D categorization scheme. The novel element of this scheme is that it does not rely heavily on exercise tolerance, as the previous scheme did, and also includes dogs in Category A that do not yet have a cardiac disease but have a risk of developing it, i.e. predisposed breeds such as Cavalier King Charles Spaniels. Category B includes dogs with mild heart disease; B1 being reserved for dogs without and B2 with cardiomegaly, but no history of present or past heart failure. Category C includes dogs in heart failure, either one with need of hospitalization (C1) or treated at home (C2). Category D is reserved for dogs in refractory heart failure and divided in D1 and D2 similar to category C. Categorized dogs can be moved from one to another category, depending on the stage of the disease (25).
Class A dogs are those that are predisposed to MMVD, such as specific breeds, and geriatric dogs, and have no signs of disease at the point of diagnosis. The consensus is that these dogs at risk should be screened regularly for the disease (auscultation and additional echocardiography for certain breeds like Cavalier King Charles Spaniels).
Class B patients are divided into two groups. B1 patients have cardiac disease but do not have clinical signs or cardiomegaly. For this group of dogs, there is no recommended treatment at this time that would prolong this asymptomatic period. At this stage, only periodic assessment is recommended in order to identify dogs that have a progression of the disease.
B2 patients have mitral regurgitation and cardiomegaly, but no clinical signs. As mentioned above, the disease in these dogs progresses in a non-linear manner; the most rapid change is observed during the last six to twelve months prior to the onset of CHF and during CHF (20, 22, 30, 31). There is no consensus for this group of patients regarding whether or not a therapy might be beneficial. Two studies showed that long-term treatment with enalapril in asymptomatic dogs with MVD and MR did not or modestly delayed the onset of heart failure regardless of whether or not cardiomegaly was present at initiation of the study (27, 28). Despite the lack of consensus, some use angiotensin-converting enzyme inhibitors (ACE-I) in this period of the disease, as it was shown in some studies in dogs and people to have some beneficial effect (28, 29).
Other drugs that might be used at this stage of the disease, such as inodilators (i.e. pimobendan), mineralocorticoid receptor blocker (i.e. spironolactone), or beta-adenergic receptor blockers, have no proven beneficial effect on reducing progression of the disease; therefore, there is no consent of using any of these drugs (26).
Class C is reserved for dogs having signs of heart failure at present or in the past, such as signs of congestion and edema or low output signs (exercise intolerance, weakness, syncope).
C1 class represents dogs having an acute episode of heart failure, secondary to severe MMVD, and needing to be hospitalized for stabilization. This may be the first episode of presenting heart failure signs or is a worsening of an already treated dog for CHF. This crisis may be due to a chordal rupture, the onset of arrhythmia, atrial rupture or a stressful event. The ACVIM panel suggested the following pharmacological management: beside the oxygen supplementation and nursing care, furosemide 1–4 mg/kg IV, IM or SC as bolus or 1 mg/kg CRI (constant rate) infusion, the latest being reserved for dogs not responding to a bolus injection (32). My personal experience is to use higher doses of furosemide such as 4–8 mg/kg in severe pulmonary edema cases; the dose depends on the kidney status of the animal, the amount of water taken and age. Monitoring respiratory rate, ECG, urine output and drinking is essential. The crucial note here is if the animal is too stressed because of dyspnea and it is obvious that cardiogenic edema is most likely, I do not stress the dog with radiography, but rather wait until it is at least stable to do a dorso-ventral view. The ACVIM panelists suggest also using pimobendan at 0.25–0.3 mg/kg q12 h (26). Other drugs, such as ACE-I, dobutamine, and hydralazine, did not meet consensus by the group at this stage of the disease (26).
Class C2 represents dogs that have clinical signs of CHF, but are stable enough to go home on therapy. The most common and suggested therapy by panelists is furosemide (1–2 mg /kg q12 h to 4–6 mg/kg q8 h orally), ACE-I (dose depends of the drug used), pimobendan (0.25–0.3 mg/kg q12 h) (26). For the following drugs, no consensus has been reached but many cardiologists use spironolactone for its diuretic, potassium-sparing and presumably anti-fibrotic properties, digoxin (0.22 mg/m2) for rate control, beta adrenergic blockers in cases of atrial fibrillation to control the ventricular rate, or ventricular arrhythmias. Diltiazem can be used as well for the rate control in atrial fibrillation. Other drugs that can be utilized and are used by some veterinarians are amlodipine (up to 0.1 mg/kg q12 h, needs to be titrated and monitor blood pressure), hydrochlorthiazide (2–4 mg/kg q12 h) and torsemide (0.2mg/kg q12-24 h) instead of furosemide. These last three drugs are usually reserved for refractory heart failure cases. Care should be taken not to use beta-blockers until the patient is stable, because these agents can exacerbate the signs of overt heart failure.
Class D patients are those that have more than one episode of heart failure and have been treated with relapses or are refractory to conventional treatment, or have signs of low output failure (weakness, syncope or exercise intolerance).
Class D1 represents dogs with acute worsening of CHF and needing hospitalization. They have clinical signs of congestive and or/low output heart failure. These patients require optimal care in terms of stabilizing their hemodynamic status. Usually they need pleural or abdominal centesis, oxygen, nursing care. They need furosemide, in the already mentioned doses in C1 patients and pimobendan for inotropic an afterload reducing support. Amlodipine may be used for afterload reduction with careful arterial pressure monitoring.
Class D2 patients are similar to D1, they have signs of congestion or low output failure, and have had relapses of it but are suitable for home treatment. The recommended pharmaceutical treatment is furosemide (1–6 mg/kg q8-12 h) with careful monitoring of renal parameters; mild azotemia is unavoidable and well tolerated. Diuresis can be increased by higher dosage or increased frequency of application, also in refractory cases furosemide can be given by SQ injection by the owner instead of a tablet. In these cases, additional diuretics are added like hydrochlorthiazide (1–2 mg q12–24 h), spironolactone (2 mg /kg q24h) or torsemide (0.1 × dose of furosemide) (26, 32). To this drug regimen, other drugs can be added, such as digoxin, beta-blockers, cough suppressants, bronchodilators, sildenafil, but no consensus has been reached on them (26).
With this polypharmacological management, patients can be supported for quite some time, depending of the state at the first presentation, age, kidney status and owner care.
Prognostic information can be gained also from the serial measurements of high-sensitivity cardiac troponin I and NT-proBNP (N-terminal pro B-type natriuretic peptide). High-sensitivity cardiac troponin I, left-ventricular end-systolic diameter normalized to body weight, heart rate and age were independently associated with decreased survival time (33).
Dogs with severe mitral regurgitation have poor prognosis even with all the pharmacological options that currently exist. Recent improvements in cardiopulmonary bypass techniques have enabled its use in small breed dogs (34, 35). In the case of prosthetic valves, matching the size of the valve and conquering thrombosis is essential for long-term prognosis (36). Recently, successful techniques for mitral valve repair with annuloplasty and chordal replacement have been utilized, which enables long-term survival for severe MMVD patients (37). Costs and availability are the major drawbacks of this option.
There are still more questions than answers in this disease (38).
More studies regarding the effect of various therapies on the disease progression and outcome are in progress. Disease pathways are studied to help understand molecular pathophysiology and discover possible drug interactions. Genetic studies are evolving for uncovering hereditary aspects of the disease and suggesting possible breeding perspectives that would both help to produce more healthy individuals and combat the disease with means of gene replacement therapy.
Mitral valve disease has become a widely recognized disease that enables early diagnosis and treatment. A wide range of pharmacological options for treatment of MMVD provide reasonable quality of life and survival. Surgical repair of the mitral valve provides an option for severely ill animals.
© 2015 Domanjko Petrič A. This is an open-access article published under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
Macedonian Veterinary Review. Volume 38, Issue 1, Pages 13-20, p-ISSN 1409-7621, e-ISSN 1857-7415, DOI: 10.14432/j.macvetrev.2014.11.026, 2015