Mac Vet Rev 2015; 38 (1): 119 - 122
 10.14432/j.macvetrev.2015.02.039
10.14432/j.macvetrev.2015.02.039
Received: 18 November 2014
Received in revised form: 19 January 2015
Accepted: 02 February 2015
Available Online First: 13 February 2015
Published on: 15 March 2015
Keywords: Indian crested porcupine (Hystrix indica), pathology, quill injury, pleuritis, septicaemia
Indian crested porcupine (Hystrix indica, Kerr, 1792) is a member of the family of Old World porcupines (Hystricidae), which belong to the order Rodentia (1). These animals are large and heavy, with a total length of almost 1 m and a weight of 10-17 kg. The neck and shoulders are covered with multiple layers of quills, exploited in its defensive behavior. Indeed, when attacked, the Indian Crested porcupine uses the tactic of hind or caudal defense; it faces away from the adversary, raises its quills and rattles the hollow quills on its tail (3). If the predator persists past these threats, the porcupine launches a backwards assault, hoping to stab its attacker with its quills. It does this so effectively that most brushes between a porcupine and its predators end in the predator’s death or severe injury (2). Quill injuries are more frequently attributed to the North American porcupine (Erethizon dorsatum), a member of the New World porcupine family (Erethizontidae), with dogs, coyotes and wolves most commonly involved in such encounters. Severe pain, local tissue trauma, infection of deep tissues, quill migration into joints or vital organs and complications associated with penetration into thorax or abdomen are frequent consequences of those assaults (4-12).
We describe unusual pathomorphological lesions in an Indian crested porcupine from the Ljubljana Zoo, which died three weeks after perforative quill injury of the thoracic wall.
An Indian crested porcupine was dissected at the Institute of Pathology, Forensic and Administrative Veterinary Medicine of the Veterinary Faculty in Ljubljana. Representative specimens of the thoracic wall, costal pleura, spleen, liver, small and large intestine, lungs and kidneys were fixed in 10% neutral buffered formalin for 24 hours, routinely embedded in paraffin, sectioned at 4 μm and stained with hematoxylin and eosin (HE).
Samples of the subcutaneous abscess, exudate from the thoracic cavity, spleen, liver, small intestine, lungs, heart and kidneys were taken for bacteriological culture. The samples were inoculated on nutrient agar (Oxoid, Hampshire, UK) supplemented with 5% sheep blood, Drigalski agar and Sabouraud dextrose agar (Oxoid, Basingstoke, UK) with chloramphenicol (100 mg/l) and incubated at 37°C for 48 hours.
An adult, 10-year old alpha male Indian crested porcupine, weighing 14.5 kg from the Ljubljana Zoo suddenly died three weeks after a fight with a younger male from its own family. Immediately after the fight, the porcupine was treated with terramycin (oxytetracyclin) and supportive vitamin therapy.
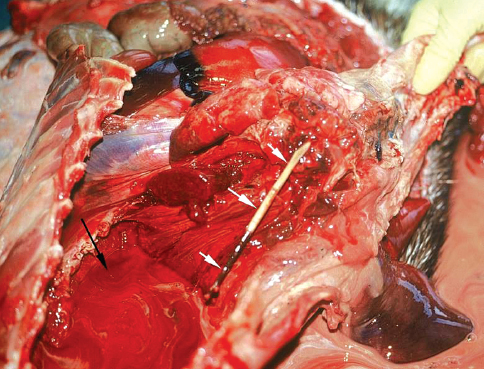
At the necropsy, an oval subcutaneous abscess, measuring 7 cm x 4 cm x 2 cm, filled with white, creamy pus, was situated in the right costal region. Close to the abscess, a round-shaped perforation with purulent inflamed edges was observed in the intercostal muscles near the 6th right rib. An abscess, containing 0.5 litres of red-whitish, creamy pus and a large red clot, was formed in the thoracic cavity. A 13 cm long quill of an Indian crested porcupine was stuck in the right cranial lung lobe, which was diffusely necrotic (Fig. 1). The other lobes of the right lung were firm and the parenchyma contained purulent exudate, the left lungs were atelectatic and multifocally emphysematous. The pulmonary pleura was diffusely covered with a thick fibrin layer.
Figure 1 Thoracic cavity. Red-whitish, creamy pus filled the left pleural cavity (black arrow). A quill of an Indian crested porcupine is stuck in the right cranial lung lobe (white arrows)
The parietal and the visceral layer of the pericardium were firmly adhered and an abscess measuring 2 cm x 1 cm x 0.5 cm was observed between the two layers. The right heart chambers were severely dilated. Numerous petechial hemorrhages, scattered throughout the kidney cortex, diffuse catarrhal enteritis and severe liver and spleen congestion were also observed.
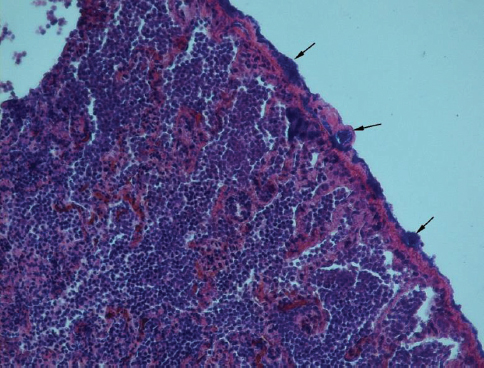
Microscopically, the alveoli and bronchi of the right lung were diffusely infiltrated with numerous heterophils and some macrophages; small multifocal bacterial colonies were also observed. The parenchyma of the left lung was atelectatic and multifocally emphysematous. The pleura was multifocally covered with a thick fibrin layer, diffusely infiltrated by heterophils, few macrophages, erythrocytes and numerous bacteria. A thick band of parenchyma beneath the pleura was densely infiltrated with macrophages and heterophils (Fig. 2). The pericardium was thickened due to granulation tissue proliferation and diffusely adhered to the epicardium. Focally, there was an abscess filled with numerous degenerative heterophils and multifocal bacterial colonies.
Figure 2 Lung. Pleura and a thick band of lung parenchyma beneath the pleura are densely infiltrated with heterophils, macrophages and numerous bacteria (arrows). HE staining, x 100
Histopathological examination of other organs revealed several lesions consistent with septicemia, i.e. a multifocal purulent hepatitis and nephritis, marked lymphocyte depletion in the spleen and acute catarrhal desquamative enteritis.
Bacteriological cultures of the spleen, lungs, heart and pus on blood agar yielded abundant growth of two types of haemolytic colonies, both Gram-positive cocci. The predominant colonies were smooth, 2-3 mm in diameter, catalase and coagulase positive and were agglutinated with rapid test Monostaph plus (Bionor Laboratories AS, Klostergata, Norway). The biochemical characteristics were evaluated using the commercial kit API Staph (bioMerieux, Marcy I’Etoile, France) and the strain was determined as Staphylococcus aureus. The smaller (1-1.5 mm) colonies were catalase negative, Gram-positive cocci and therefore suspected to be streptococci.
The biochemical characteristics were evaluated using the commercial kit API Strep and the strain was determined as Streptococcus agalactiae. The culture was serologically typed according to the Lancefield classification system using the Streptococcal grouping kit (Oxoid, Basingstoke, UK) and classified in group B. Culture from the pus also yielded a few colonies of nonhaemolytic coryneform bacteria.
The samples from the kidney, liver and intestine were bacteriologically negative.
Despite a wide geographic range of the Indian crested porcupine (13), there is absence of literature data on injuries. All reported cases of porcupine quill injuries were related to a relative of the Indian crested porcupine, the North American porcupine (Erethizon dorsatum). In this species, the tip of its quill is covered with backward-pointing barbs and beyond them the shaft is smooth and hollow, which forces the quill, stuck in the tissue, to migrate into deeper layers (14). In injured dogs, porcupine quills are commonly seen in the external head and neck region, followed by the oral cavity, and are less often found in limbs and the truncal region. Inflammation or discharge and less often lameness and ocular signs occur in 10.8% of all injured dogs. Only in one case, a pneumothorax caused by quills in the cranial mediastinum and cranial lung lobe was reported (11).
Porcupine quills are not inert; they may harbor bacteria or act directly evoking septic or sterile foreign body reaction (8). Staphylococcus aureus (9, 10, 12) and Staphylococcus intermedius were isolated from ocular and orbital injuries (8), septic arthritis (10) and vertebral canal porcupine quill injury (12) in dogs and also septic tenosynovitis in the horse (9), all caused by a North American porcupine quill injury. A septic pleuritis, purulent bronchopneumonia with pyothorax, adhesive pericarditis and subsequent septicemia caused by Staphylococcus aureus, Streptococcus agalactiae and Corynebacterium sp. were observed in our case. Liver, kidney and intestine were bacteriologically negative, most probably due to distribution of the lesions in these organs and less likely due to previous antibiotic treatment.
© 2015 Švara T. This is an open-access article published under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The authors wish to thank the ZOO Ljubljana for their cooperation and permission for the publication of data.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
Macedonian Veterinary Review. Volume 38, Issue 1, Pages 119-122, p-ISSN 1409-7621, e-ISSN 1857-7415, DOI: 10.14432/j.macvetrev.2015.02.039, 2015