Mac Vet Rev 2016; 39 (1): 83 - 90
 10.1515/macvetrev-2016-0075
10.1515/macvetrev-2016-0075
Received: 10 October 2015
Received in revised form: 11 January 2016
Accepted: 20 January 2016
Available Online First: 01 February 2016
Published on: 15 March 2016
Keywords: dogs, pulmonary arterial hypertension, respiratory disease, tricuspid regurgitation
In veterinary medicine, pulmonary arterial hypertension (PAH) is defined as pulmonary arterial systolic pressure greater than 25 mmHg (1). Right-heart catheterization is considered the “gold standard” in order to diagnose PAH (2, 3, 4). However it is rarely performed in veterinary medicine (1, 3, 4). In the absence of right ventricular (RV) outflow tract obstruction (e.g. pulmonary stenosis) or significant right-sided volume overload (e.g. tricuspid valve dysplasia), pulmonary arterial pressure can be inferred non-invasively with Doppler echocardiography, either by calculation of the maximal velocity of the regurgitant flow across the tricuspid (systolic pulmonary arterial pressure) or across the pulmonary valve (diastolic pulmonary arterial pressure) using the modified Bernoulli equation (4, 5, 6).
The severity of PAH is classified as mild, moderate, and severe based on the estimated pulmonary arterial pressure, with slight variations in cut off values among reports, in dogs affected by cardiovascular diseases (6, 7, 8).
PAH may occur through three mechanisms: increased left atrial pressure, increased pulmonary blood flow, and increased pulmonary vascular resistance. The pathophysiology of PAH is multifactorial and results from an imbalance of endogenous and exogenous pulmonary artery vasodilators and vasoconstrictors; this disequilibrium causes vasoconstriction, vascular smooth muscle cell proliferation and thrombosis, leading to an increased pulmonary vascular resistance in PAH (9, 10).
In people, chronic obstructive airway disease is one of the most common pulmonary causes of PAH (11). Chronic obstructive airway disease may decrease the partial pressure of alveolar oxygen, which can result in hypoxia. In contrast to the systemic vasculature, which responds to hypoxia with vasodilatation to better perfuse hypoxic tissue, the pulmonary vasculature responds to hypoxia by pulmonic arterial vasoconstriction, which subsequently increases the pulmonary pressure (6). Few data is available on the PAH prevalence in dogs, except for selected conditions such as canine heartworm disease, left-sided heart failure and Angiostrongylus vasorum infection (12, 13, 14, 15, 16, 17)
Recently, some authors evidenced an association of pulmonary hypertension and increase serum CRP (C-reactive protein) concentrations in dogs affected by heartworm disease (12). Interestingly, the CRP concentration relates to the severity of endothelial arteritis, and not as a result of heartworm disease itself (12). The CRP concentration was still high even following adulticide treatment, and this underlined the possibility that CRP may be used as an early biomarker of pulmonary hypertension (12).
In veterinary medicine, lung disease, such as chronic pneumonia and lung fibrosis, chronic bronchitis, bronchiectasis, and upper respiratory disease such as tracheal collapse and laryngeal paralysis, have been associated with sustained or intermittent hypoxia and subsequent PAH development (10). PAH in dogs occurs mostly in patients with very advanced disease or those with predisposing conditions (9, 10). However, there are no known studies assessing the prevalence of PAH in dogs with bronchial and/or upper respiratory disease. The aim of this study was to assess the prevalence of PAH in dogs with bronchial and/or upper respiratory disease.
The medical records of 1,063 dogs referred for cardiovascular investigation at the Cardiology Unit of the Department of Veterinary Science and Public Health between January 2009 and May 2013 were retrospectively reviewed. Only first visit cases were included in the study.
Inclusion criteria were: complete clinical records, radiographic, echocardiographic, a confirmed diagnosis by endoscopic examination of bronchial and/or upper respiratory disease and negative Dirofilaria immitis antigen test.
Exclusion criteria were: any cardiac and/or systemic disease that may cause PAH, except for mild mitral valve disease; diagnosis of Angiostrongylus vasorum, achieved using a Baermann faecal test performed at a veterinary diagnostic laboratory, or by detection of L1 larvae on a direct faecal smear or bronchoalveolar lavage sample by a trained operator. The signalment, clinical history, and clinical signs (cough, dyspnoea, syncope, asthenia, weight loss, snoring, and reverse sneezing) were recorded.
Echocardiography was performed using an ultrasound system (MyLab 50, ESAOTE, Florence, Italy) equipped with a phased array transducer (7.5−10 MHz for small dogs, 5−7.5 MHz for medium dogs, and 2.5−3 MHz for large dogs and Doppler studies). Examinations were performed in awake dogs in left and right lateral recumbency, as recommended by the American Society of Echocardiography (18).
The following echocardiographic parameters were evaluated:
1. Presence/absence of RV hypertrophy and/or dilation in the right parasternal long axis 4-chamber and short axis views at the level of the papillary muscle. The RV wall thickness was considered increased (RV hypertrophy) if it was greater than half the thickness of the left ventricular free wall (1). The RV chamber size was considered normal if it was smaller than or equal to one-half of the left ventricular thickness, mildly enlarged if greater than or equal to one-half the left ventricular thickness, or severely enlarged if greater than the left ventricle (5).
2. Presence/absence of flat or paradoxical interventricular septal motion in the right parasternal short axis and/or in M-mode at the level of the papillary muscle (10).
3. Presence/absence of main pulmonary artery enlargement based on the ratio between the diameters of the main pulmonary artery and the aorta (PA:AO ratio): a ratio greater than 0.98 was considered enlarged (1).
1. Presence/absence of tricuspid regurgitation (TR): the TR systolic peak velocity (m/s) and peak systolic gradient (mmHg) were measured when present.
2. Presence/absence of pulmonic insufficiency (PI): the PI diastolic peak velocity (m/s) and peak diastolic gradient (mmHg) were measured when present. The presence and severity of PI were assessed through colour flow mapping, and the extension of the regurgitation jet and its width at the origin were evaluated (20).
3. Pulmonary artery systolic flow profiles: Type I (normal) was defined as a symmetric profile and a rounded systolic peak; type II (mild and moderate PAH) as a peak velocity occurring during early systole and a long deceleration phase (asymmetric profile); and type III (severe PAH) was defined as having a notch in the deceleration phase (1).
4. Systolic time intervals: The acceleration time (AT), defined as the time to peak pulmonary artery flow velocity; RV ejection time (ET); and AT:ET ratio were assessed (21).
Doppler flow interrogations of the TR and PI jets were used to estimate the systolic and diastolic pulmonary arterial pressure respectively, allowing diagnosis and quantification of PAH (10). PAH was diagnosed when the TR systolic peak velocity (m/s) was greater than 2.8 m/s; the TR systolic peak velocity (m/s) and peak systolic gradient (mmHg) were used to classify the PAH severity (Table 1) (1, 4). The presence of PI with a velocity >2.2 m/s was considered suggestive of diastolic PAH (1, 4).
Table 1. Classification of pulmonary hypertension based on TR (tricuspid regurgitation) peak systolic velocity and TR gradient (1). (TR: tricuspid regurgitation)
If TR/PI were absent, then PAH was considered possible when two or more of the following echocardiographic findings were recorded:
1. Presence of RV hypertrophy and/or dilation (5, 19)
2. Presence of main pulmonary artery enlargement (PA:AO ratio > 0.98) (1)
3. Presence of type II or III pulmonary artery systolic flow profile (1)
4. AT:ET < 0.31 and/or AT < 58 ms (21)
Endoscopy was performed using either a rigid instrument equipped with a 18-cm optical length, 2.7-mm thickness, (Karl Storz Hopkins II, Dr. Karl-Storz-Straße 34 Tuttlingen, Germany), 1-ccd camera (Wolf Endocam 551, Pforzheimer-Straße 32, 75438 Knittlingen, Germany), and xenon light source (Storz Xenon Nova 20131520, Dr. Karl-Storz-Straße 34 Tuttlingen, Germany) for examination of the nasal cavity, or a flexible video endoscope (4.9-mm diameter and 2-mm channel size, Fujinon Videobronchoscope EB-270 S7-3, Akasaka 9-chome, Minato-ku, Tokyo 107-0052, Japan) for examination of other respiratory airways.
The Shapiro–Wilk test was used to verify normal distribution. Normally distributed data were expressed as the mean ± standard deviation. For data not normally distributed, the median and interquartile (IQR (25th to 75th percentile)) were calculated. Data were analyzed using statistical software (JMP version 7, JMP Headquarters, SAS Institute, Cary, NC, USA 27513).
Fifty-two clinical records fulfilled the inclusion criteria (35 males and 17 females), and represented 4.9 % of the total referral patients seen at the Cardiology Unit of the Department of Veterinary Science and Public Health between January 2009 and May 2013. Fourteen breeds were represented: 10 English Bulldogs (19%) resulted the prevalent, 7 males (70%) and 3 females (3%), followed by 8 crossbreeds dogs (15%), 5 males (62.5%) and 3 females (37.5%), 8 French Bulldogs (15%), 7 males (87.5%) and 1 female (12.5%) and 6 Yorkshire Terriers (11%), 2 males (33.3%) and 4 females (66.6%). The age ranged from 0.8 to 16 years (median 7 years; IQR: 3−12.25 years) and the weight from 2 to 40 kg (median 12 kg; IQR: 7.35−18 kg). All dogs showed at least one clinical sign: cough (50.1%), dyspnoea (50.1%), snoring (30.1%), exercise intolerance (15%), weight loss (9.4%), reverse sneeze (5.2%), and syncope (5.6%). Twenty-eight dogs (54%) showed more than one clinical sign simultaneously. The most common associations of symptoms were cough, dyspnoea and exercise intolerance (10.7%), cough and dyspnoea (21.4%), dyspnoea and snoring (10.7%).
Seventeen dogs (33%; 8 females and 9 males) were diagnosed with bronchial disease (9 chronic bronchitis, 6 chronic bronchitis and bronchial collapse, 2 bronchial collapse). The prevalence on the total population referred was 1.6 %. Crossbreed dogs were the most represented (39%); the age ranged from 1 to 15 years (median 12 years; IQR: 11−13 years) and the weight from 3 to 16 kg (median 8 kg; IQR: 4−13.25 kg).
Thirty dogs (56.6%; 8 females and 22 males) were diagnosed with upper respiratory disease. Twenty-one of them resulted affected by brachycephalic airway obstructive syndrome (BAOS) (70 %; 5 female and 16 male), 3 by laryngeal paralysis, 2 by tracheal collapse, and 1 by laryngeal collapse; 3 dogs exhibited multiple upper respiratory disease simultaneously. The prevalence on the total population referred was 2.8 %. The most represented breeds were English and French Bulldogs (57%). The age ranged from 0.8 to 16 years (median 3.5 years; IQR: 3−10.25 years), and the weight ranged from 2 to 40 kg (median 13.85 kg; IQR: 10−21 kg). In the BAOS group specifically, the age ranged from 0.11 to 12 years (median 3 years; IQR: 2−4 years) and the weight from 8 to 26 kg (median 14 kg; IQR: 12−21 kg). Five dogs (9.5%; 1 female and 4 males), exhibited upper respiratory disease and bronchial disease simultaneously, 0.5 % the prevalence of this group on the total population referred to the Cardiology Unit during the study time.
Mild RV enlargement was found in 4 dogs (7.5%) and mild RV hypertrophy in 2 dogs (3.8%). One dog (1.9%) exhibited both RV hypertrophy and dilation simultaneously. No dog presented flat or paradoxical interventricular septal motion or main pulmonary artery enlargement.
TR was observed in 15 dogs (29%). The TR peak systolic velocity ranged from 1.51 m/s to 4.02 m/s (mean 2.62 ± 0.71 m/s), and the TR systolic gradient ranged from 9.10 mmHg to 64.60 mmHg (median 23.90 mmHg; IQR: 17.88−30.15 mmHg).
No dog showed pulmonary insufficiency. Type II pulmonary artery systolic flow profile was found in 2 dogs (3.8%) and was associated with mild RV hypertrophy in both. No dog presented an AT: ET ratio equal to or less than 0.31, and none exhibited an AT equal to or less than 58 ms. The mean AT: ET ratio was 0.48 ± 0.04, and the mean AT was 83.08±14.24 ms.
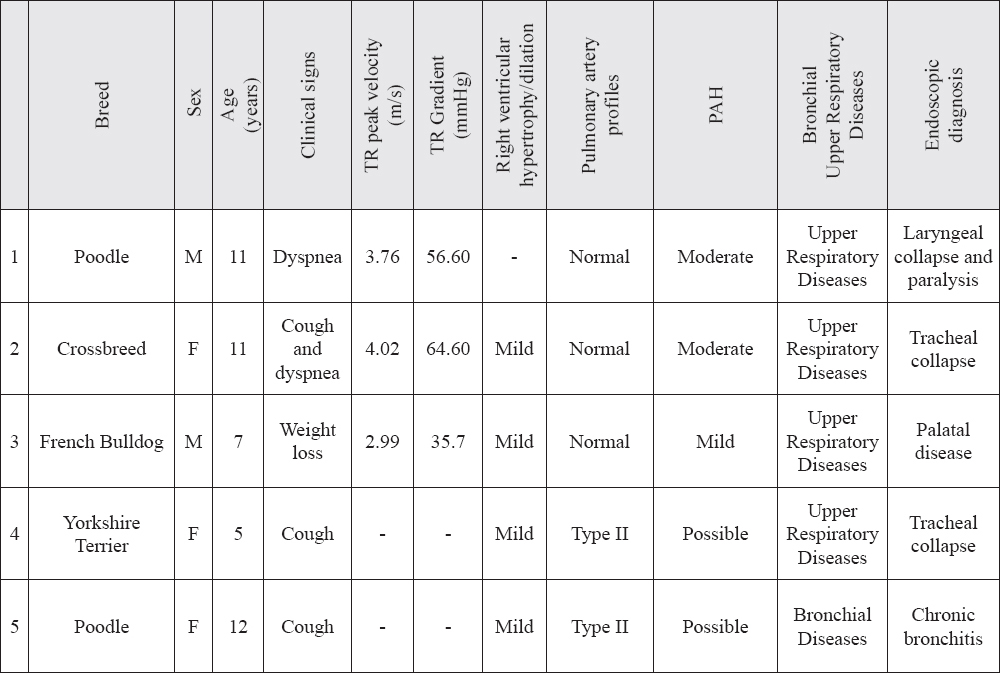
PAH was diagnosed in 3 dogs (5.7%) based on a TR peak systolic velocity >2.8 m/s. All three dogs were diagnosed with upper respiratory disease; therefore, the prevalence of PAH in this subgroup was 10%. Two dogs (one with bronchial disease and one with upper respiratory pathology) were considered likely to have PAH based on the presence of secondary specific echocardiographic findings. A total of 5 dogs (9.4%) had confirmed or probable PAH (Table 2), the prevalence in the overall referral population being 0.5 % and 1 % of dogs with valvular disease.
Table 2. Signalment, clinical signs, echocardiographic and Doppler data, PAH severity and endoscopic diagnosis of 5 dogs affected by PAH. (F: female; M: male; TR: tricuspid regurgitation)
All applicable international, national, and institutional guidelines for the care and use of animals were followed. All procedures performed in studies involving animals were in accordance with the ethical standards of the institution or practice at which the studies were conducted. For this type of study, formal consent was not required.
1. Kellihan, H.B., Stepien, R.L. (2010). Pulmonary hypertension in dogs: diagnosis and therapy. Vet Clin Small Anim. 40, 623-641. http://dx.doi.org/10.1016/j.cvsm.2010.03.011 PMid:20610015
2. Galiè, N., Hoeper, M., Humbert, M. et al. (2009). Guidelines for the diagnosis and treatment of pulmonary hypertension. European Heart Journal 30, 2493-2537. http://dx.doi.org/10.1093/eurheartj/ehp297 PMid:19713419
3. Soydan, L.C., Kellihan, H.B., Bates, L.B., Stepien, R.L., Consigny, D.W., Bellofiore, A., Francois, C.J., Chesler, N.C. (2015). Accuracy of doppler echocardiographic estimates of pulmonary artery pressures in a canine model of pulmonary hypertension. Journal of Veterinary Cardiology 17, 13 – 24. http://dx.doi.org/10.1016/j.jvc.2014.10.004 PMid:25601540
4. Borgeat, K., Sudunagunta, S., Kaye, B., Stern, J., Luis Fuentes, V., Connolly, D. J. (2015). Retrospective evaluation of moderate-to-severe pulmonary hypertension in dogs naturally infected with angiostrongylus vasorum. Journal of Small Animal Practice 56, 196–202. http://dx.doi.org/10.1111/jsap.12309 PMid:25483150
5. Johnson, L., Boon, J., Orton, E.C. (1999). Clinical characteristic of 53 dogs with Doppler - derived evidence of pulmonary hypertension 1992–1996. Journal of Veterinary Internal Medicine 13, 440–444. PMid:10499728
6. Kellihan, H.B., Stepien, R.L. (2012). Pulmonary hypertension in canine degenerative mitral valve disease. Journal of Veterinary Cardiology 14,149–164.
http://dx.doi.org/10.1016/j.jvc.2012.01.001 PMid:22364721
7. Pyle, R.L., Abbott, J., Maclean, H. (2004). Pulmonary hypertension and cardiovascular sequela in 54 dogs”. International Journal of Applied Research in Veterinary Medicine 2, 99–109.
8. Serres, F.J., Chetboul, V., Tissier, R., Sampedrano, C.C., Gouni, V., Nicolle, A.P., Pouchelon, J.L. (2006). Doppler echocardiography-derived evidence of pulmonary arterial hypertension in dogs with degenerative mitral valve disease: 86 cases (2001–2005). Journal of the American Veterinary Medical Association 229, 1772–1778. http://dx.doi.org/10.2460/javma.229.11.1772 PMid:17144824
9. Johnson, L.R., Hamlin, R.L. (1995). Recognition and treatment of pulmonary hypertension. In: Bonagura J.R.D. (Ed.), Kirk’s Current Veterinary Therapy XII (pp 887 – 892). Philadelphia USA: WB Saunders.
10. Campbell, F.E. (2007). Cardiac effects of pulmonary disease. Veterinary Clinics North America Small Animal Practice 37. 949-962. http://dx.doi.org/10.1016/j.cvsm.2007.05.006 PMid:17693208
11. Mc Laughlin. V.V., Rich. S. (2000). Corpulmonale. In: Braunwald E, Zipes DP, Libby P. (Ed.), Heartdisease: a textbook of cardiovascular medicine. 6th Edition. (pp 1936-1956). Philadelphia USA: WB Saunders.
12. Venco, L., Milhaylova, L., Boon, J.A. (2014). Right pulmonary artery distensibility index (RPAD index). A field study of an echocardiographic method to detect earl development of pulmonary hypertension and its severity even in the absence of regurgitant jets for Doppler evaluation in heartworm-infected dogs. Vet Parasitol. 206, 60-6. http://dx.doi.org/10.1016/j.vetpar.2014.08.016 PMid:25218885
13. Swann, J., Sudunagunta, S., Covey, H.L., English, K., Hendricks, A., Connolly, D.J. (2014). Evaluation of red cell distribution width in dogs with pulmonary hypertension. Journal of Veterinary Cardiology 16, 227-235. http://dx.doi.org/10.1016/j.jvc.2014.08.003 PMid:25465342
14. Sasaki, Y., Kitagawa, H., Hirano, Y. (1992). Relationship between pulmonary arterial pressure and lesionsin the pulmonary arteries and parenchyma, and cardiac valves in canine dirofilariasis. Journal of Veterinary Medical Science 54, 739–744. http://dx.doi.org/10.1292/jvms.54.739
15. Nicolle, A.P., Chetboul, V., Tessier-Vetzel, D., Sampedrano, C.C., Aletti, E., Pouchelon, J.L. (2006). Severe pulmonary arterial hypertension due to Angiostrongylosu svasorum in a dog. The Canadian Veterinary Journal 47, 792-795. PMid:16933559 PMCid:PMC1524835
16. Traversa, D., Di Cesare, A., Meloni, S., Frangipane di Regalbono, A., Milillo, P., Pampurini, F., Venco, L. (2013). Canine angiostrongylosis in Italy: prevalence of Angiostrongylus vasorum in dogs with compatible clinical pictures. Parasitology Research 112, 2473-2480. http://dx.doi.org/10.1007/s00436-013-3412-5 PMid:23595212 PMCid:PMC3683398
17. Borgarelli, M., Abbott, J., Braz-Ruivo, L., Chiavegato, D., Crosara, S., Lamb, K., Ljungvall, I., Poggi, M., Santilli, R.A., Haggstrom, J. (2015). Prevalence and prognostic importance of pulmonary hypertension in dogs with myxomatous mitral valve disease. Journal of Veterinary Internal Medicine 29, 569–574. http://dx.doi.org/10.1111/jvim.12564 PMid:25818210
18. Thomas, W.P., Gaber, C.E., Jacobs, G.J., Kaplan, P.M., Lombard, C.W., Moise, N.S., Moses, B.L. (1993). Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. Journal of Veterinary Internal Medicine 7, 247-252. http://dx.doi.org/10.1111/j.1939-1676.1993.tb01015.x
19. Boon, J.A. (1998). Evaluation of size, function and hemodynamics. In: Boon J.A. (Ed.), Manual of veterinary echocardiography (pp. 151–260). Williams & Wilkins Co, Baltimore. PMid:9654462
20. Cooper, J.W., Nanda, N.C., Philpot, E.F., Fan, P. (1989). Evaluation of valvular regurgitation by colour Doppler. Journal of the American Society of Echocardiography 2, 56-66. http://dx.doi.org/10.1016/S0894-7317(89)80030-6
21. Schober, K.E., Baade, H. (2006). Doppler echocardiographic prediction of pulmonary hypertensionin West Highland White Terriers with chronic pulmonary disease. Journal of Veterinary Internal Medicine 20, 912-920. http://dx.doi.org/10.1111/j.1939-1676.2006.tb01805.x
22. Glaus, T., Schnyder, M., Dennler, M., Tschuor, F., Wenger, M., Sieber-Ruckstuhl, N. (2010). Natural infection with Angiostrongylus vasorum: characterisation of 3 dogs with pulmonary hypertension. Schweizer Archiv für,Tierheilkunde152, 331-338. http://dx.doi.org/10.1024/0036-7281/a000076 PMid:20582899
23. Estèves, I., Tessier, D., Dandrieux, J., Polack, B., Carlos, C., Boulanger, V., Muller, C., Pouchelon, J.L., Chetboul, V. (2004). Reversible pulmonary hypertension presenting simultaneously with an atrial septal defect and angiostrongylosis in a dog. Journal of Small Animal Practice 45, 206-209. http://dx.doi.org/10.1111/j.1748-5827.2004.tb00226.x PMid:15116890
24. Matos, J. M., Schnyder, M., Bektas, R., Makara, M., Kutter, A., Jenni, S., Deplazes, P., Glaus, T. (2012). Recruitment of arteriovenous pulmonary shunts may attenuate the development of pulmonary hypertension in dogs experimentally infected with Angiostrongylus vasorum. Journal of Veterinary Cardiology 14, 313-322. http://dx.doi.org/10.1016/j.jvc.2012.01.014 PMid:22575676
25. Kuehn, N.F. (2003). Chronic bronchitis in dogs. In: L. King (Ed.), Textbook of Respiratory Diseases of the Dog and Cat (pp. 379-387). Philadelphia USA: WB Saunders.
26. Paradies, P., Spagnolo, P.P., Amato, M.E., Pulpito, D., Sassanelli, M. (2014). Doppler echocardiographic evidence of pulmonary hypertension in dogs: a retrospective clinical investigation. Veterinary Research Communication 38, 63-71. http://dx.doi.org/10.1007/s11259-013-9588-4 PMid:24414341
27. Herrtage, M.E., White, R. (2000). Management of tracheal collapse. In: J. Bonagura, RD (Ed) Kirk’s Current Veterinary Therapy XIII (pp 796-801). Philadelphia USA: WB Saunders.
28. Hendricks, J.C. (2003). Brachycephalic Airway Syndrome. In: L. King (Ed) Textbook of Respiratory Diseases of the Dog and Cat (pp. 310-318). Philadelphia USA: WB Saunders.
29. Holt, D.E., Brockman, D. (2003). Laryngeal paralysis. In: L. King (Ed) Textbook of Respiratory Diseases of the Dog and Cat (pp. 319-328). Philadelphia USA: WB Saunders.
30. Mason, R.A., Johnson, L.R. (2003). Tracheal collapse. In: L. King (Ed) Textbook of Respiratory Diseases of the Dog and Cat (pp. 346-355). Philadelphia USA: WB Saunders.
© 2016 Locatelli C. This is an open-access article publishedunder the terms of the Creative Commons Attribution License whichpermits unrestricted use, distribution, and reproduction in any medium,provided the original author and source are credited.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
Macedonian Veterinary Review. Volume 39, Issue 1, Pages 83-90, p-ISSN 1409-7621, e-ISSN 1857-7415, DOI: 10.1515/macvetrev-2016-0075, 2016