Mac Vet Rev 2017; 40 (2): 183 - 187
 10.1515/macvetrev-2017-0022
10.1515/macvetrev-2017-0022
Received: 03 April 2017
Received in revised form: 27 May 2017
Accepted: 08 June 2017
Available Online First: 04 July 2017
Published on: 15 October 2017
Keywords: VSD, cat, hybrid technique, defect closure, Amplatzer occluder, sizing balloon
Ventricular septal defect (VSD) is among the most common feline congenital heart malformations (1, 2). In cats, restrictive VSDs do not require treatment (3), but non-restrictive VSDs receive either palliative surgery or medical treatment to reduce pulmonary hypertension and excessive pulmonary blood flow. VSD closure has not yet been aggressively attempted in cats (4, 5).
Surgical closure of the defect is ideal for non-restrictive VSD in humans and dogs. The procedure includes open-heart surgery using cardiopulmonary bypass (6, 7) and percutaneous interventional radiology (IVR) (8, 9, 10, 11). Although open-heart surgeries have been reported in some feline cases (12, 13), extracorporeal circulation poses a significant risk in this species. In cats, small vessel size limits its use to cases of patent ductus arteriosus, through a femoral vein approach (14).
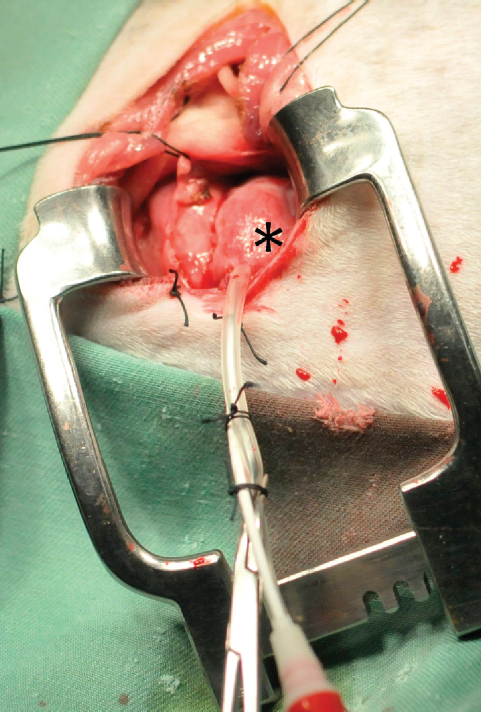
The hybrid technique used in the present study involves a combination of surgical defect occlusion and IVR, and is performed via a thoracotomy incision, with the catheter directly inserted into the heart. The procedure is not dependent on peripheral blood vessel size, and is less invasive than open-heart surgery. Moreover, because the sheath directly punctures the right ventricle (RV) (Fig. 1), operability is improved compared to IVR. The hybrid technique combines the advantages of surgical defect occlusion and IVR.
Figure 1. The hybrid technique used in the present study. The sheath directly punctures the RV (*). Operability is markedly improved compared to IVR, because little curve is encountered and the distance from the apex of the RV to the VSD is short
In the present study, the hybrid technique was attempted for the first time in a cat with VSD. The goal of the present paper is to report the advantages and disadvantages of this technique in a cat.
A 13-month-old, 3.5-kg, female Maine Coon cat was referred to our institution for exercise intolerance and respiratory distress (day 1). Abdominal and mouth breathing with tachypnea were evident at presentation. Blood pressure (BP) was 126/82 (98) mmHg (systolic/diastolic (mean)). Transthoracic echocardiography (TTE) showed a VSD (diameter, 6.3 mm; defect border to aortic valve, 3.1 mm; defect border to tricuspid valve, 4.1 mm) and left-to-right shunt (flow rate, 4.9 m/s). Pulmonic ejection velocity was 3.3 m/s. Pulmonary blood flow to systemic blood flow ratio (Qp/Qs; calculated as stroke volume (SV) of pulmonary artery/SV of aorta) from pulsed Doppler ultrasonography was 3.82. Left ventricular dimension in diastole was 34.4 mm and E wave was 1.2 m/s. Based on these findings, the cat was diagnosed with non-restrictive VSD. Physical closure of the defect was recommended based on VSD size, the calculated flow ratio and the presence of clinical signs. Initial treatment comprised pimobendan at 0.25 mg/kg twice daily and furosemide at 2.0 mg/kg/day to treat the volume overload and congestive left heart failure. Considering the risks of open-heart surgery and IVR in cats, a hybrid defect occlusion technique using an Amplatzer (Amplatzer VSD occlusion device; Shanghai Shape Memory Alloy Co., Ltd. (SHSMA); Shanghai, PRC) occluder was selected.
A left fifth intercostal thoracotomy was performed under general inhalation anesthesia maintained with isoflurane (0.9-1.5%, Isoflurane for Animals; Intervet K.K., Tokyo, Japan) (day 5). Transesophageal echocardiography imaging (TEE) identified a 7.6-mm VSD, with an interventricular septum (IVS) of 6.9 mm around the apex, and 4.1 mm around the membranous septum. A purse string suture was placed on the vertex cordis part of the RV, transfixing an 18-G indwelling needle at the center of the purse string suture. A 0.035-inch guide wire was inserted via the indwelling needle. After removing the indwelling-needle, an 11-Fr sheath was inserted and guided by guidewire for the sheath to the RV. Under TEE monitoring, the Amplatzer VSD occlusion device (12-mm disc on LV side, 12-mm disc on RV side, 8-mm waist, 6-mm height; SHSMA) was inserted via an 11-Fr sheath through the RV. A guidewire was not necessary for the Amplatzer, because the distance from sheath to defect was very short. Distance from the edge of the LV-side disk to the aortic valve was about 2 mm. The defect was almost completely occluded, without any apparent aortic outflow tract stenosis or adverse movements of the aortic valve (Fig. 2). However, the defect was too large to achieve firm fixation, and the device was easily displaced upon moving the delivery wire. The device was therefore retrieved before detachment to avoid dislodgement. The cat recovered uneventfully and was discharged 9 days after surgery (day 14).
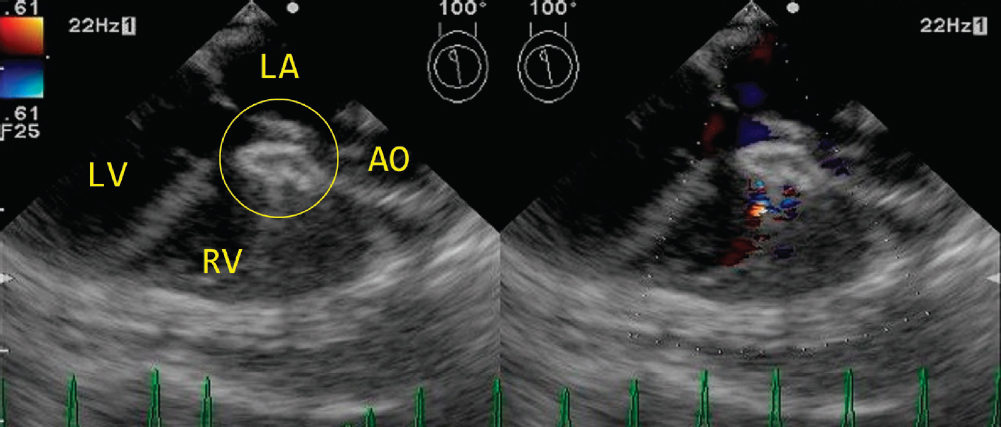
Figure 2. On day 5, the Amplatzer (circle) (12-mm disc on the left ventricle (LV) side just under the aortic valve, 12-mm disc on the RV side; waist, 8 mm; height, 6 mm) was inserted from the RV. The defect was almost completely occluded without aortic blood flow blockage, and hemodynamic exacerbation was not observed during insertion, despite protrusion of the device a few millimeters into the LV outflow tract. LA, left atrium; RV, right ventricle; AO, aorta
TTE showed that left-to-right shunt flow rate was decreased (3.0 m/s) and the E wave was increased (1.3 m/s) (day 59). RV pressure was increased and heart congestion was worsened even under pharmacotherapy (pimobendan at 0.25 mg/kg twice daily, benazepril at 0.4 mg/kg once daily, and furosemide at 2.0 mg/kg/day). Based on these clinical data, we considered that the condition of the cat was continuing to deteriorate. Hybrid defect occlusion was performed with a median sternotomy approach instead of intercostal thoracotomy (day 59), because the RV was so dilated that the position of the heart seemed to be affected during the previous surgery. Under general anesthesia, a 6-Fr sheath was placed in the RV, and using a 0.035-inch guide wire, a 7-Fr sizing balloon catheter (SBC) was inserted to measure the defect size (maximum diameter, 11 mm). An ACDO (Amplatz Canine Duct Occluder; 14-mm disc on LV side, 16-mm disc on RV side, 9-mm waist, 6-mm height; Infiniti Medical LLC, California, CA, USA) was inserted from the RV, and the distal disc was deployed in the LV while the proximal disc was deployed in the RV (Fig. 3). The distance from the edge of the LV side disk to the aortic valve was about 1 mm. Although the defect was occluded and firm fixation was achieved, exacerbation of the hemodynamics was observed after device implantation. Interference with aortic flow along with decreased LV outflow tract blood flow velocity, low peripheral oxygen saturation (<70%), bradycardia, and hypotension were observed 1-2 min after device placement. Based on these observations, the cat was deemed unsuitable for defect closure. Pulmonary artery banding was conducted instead of device placement. The cat recovered uneventfully and was discharged on day 63. Her clinical signs were limited to overall improvement, decreased tachypnea, and Qp/Qs decreased to 2.28 from TTE on day 248. However, volume overload and congestive left heart failure haven’t clearly recovered.
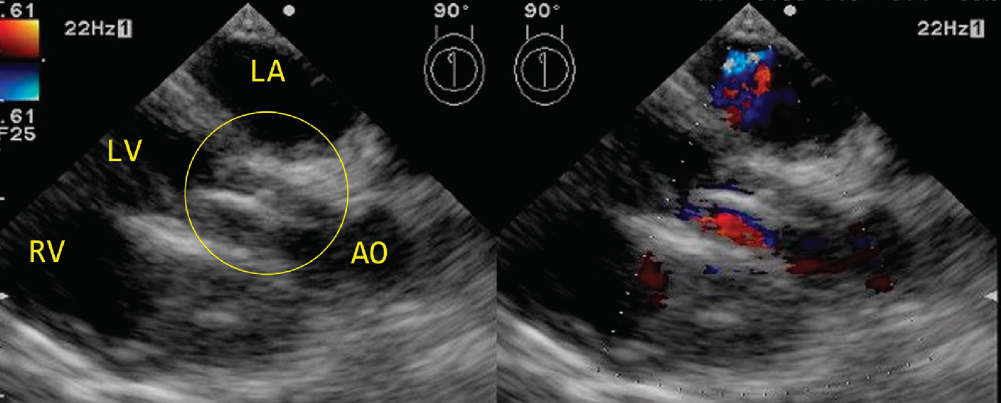
Figure 3. On day 59, the ACDO (circle) (14-mm disc on the LV side just under the aortic valve, 16-mm disc on the RV side; waist, 9 mm; height, 6 mm) was inserted from the RV. Although the defect was occluded and firm fixation was achieved, exacerbation of hemodynamics was observed after device implantation. LV, left ventricle; LA, left atrium; RV, right ventricle; AO, aorta
The attempted hybrid method offered two advantages. First, the approach is simplified by puncturing the RV with a sheath and inserting the catheter through the defect under TEE guidance. TEE allows simultaneous monitoring of the RV, LV, defect, and aorta, enabling clear visualization of the occlusion device for easy evaluation of device position. Although the devices used were either unstable or interfered with LV outflow, these issues were easily detected on TEE.
Second, advantages over open-heart surgery were observed. Even though the hybrid method was repeated within a short period of time, this cat showed no postoperative complications such as cardiac arrest, bleeding tendency, arrhythmia, or reductions in renal or liver function. The hybrid method is considered less invasive and postoperative management is less demanding compared to open-heart surgery. The hybrid method offers advantages over IVR as well (15). Although the cat weighed only 3.5 kg, an 11-Fr catheter could be inserted into the RV. With the hybrid method, a comparatively larger device was available, regardless of peripheral blood vessel size.
The disadvantages of this method include difficult evaluation of defect size and availability of appropriate occlusion devices. A significant difference in defect size was observed between TTE, TEE, and SBC - the SBC being the most reliable method in this case. Two potential reasons for this significant difference may be considered. First, the defect involved the membranous part of the interventricular septum, which is highly elastic. Second, the defect was oval in shape, not circular. TTE and TEE can only measure one dimension. However, the SBC can measure the greatest extent of the VSD, and so may offer the best method to measure the VSD defect in cats, especially for the membranous part of the defect.
Another disadvantage was that this particular method using a human or canine Amplatzer device is inappropriate for cats with very large defects. Large devices may interfere with cardiac function, such as aortic blood flow in this case. The height of the device was 6 mm, and the IVS was 4.1 mm around the membranous defect. The device thus protruded about 1 mm into the LV outflow tract, which may obstruct flow in the small feline heart. Indications depending on defect location require further investigation, since no criteria have yet been established in feline VSD suitable for device embolisation. In humans, criteria have been devised not only for suitability depending on the anatomical classification of the VSD (i.e., involving membranous or muscular parts), but also stating that a distance of at least 3 mm from the defect border to the aortic valve is necessary (16), while a distance of <4 mm to the tricuspid valve leads to complications such as postoperative arrhythmia (17). Our case met the above criteria, but LV outflow was still obstructed. Stricter criteria are thus necessary for feline VSD. In addition to the above criteria, distance from the defect border to the device edge may need to be greater and device height may need to be smaller. In the first surgery, distance from the edge of the LV side disk to the aortic valve was about 2 mm, and no hemodynamic deterioration was evident. In the second surgery, the distance was 1 mm, and hemodynamic deterioration occurred. At least 2 mm from the edge of the LV side disk to the aortic valve may thus be needed for treating VSDs in cat. In order to avoid interference with blood flow and cardiac movement, development of flatter devices with a low profile would be desirable.
Amplatzer occlusion of a large non-restrictive VSD in a cat using the herein described hybrid technique is currently not an option, because the available devices designed for humans or dogs are too large for cats. Amplatzer occlusion via the hybrid technique may still be an option for smaller non-restrictive VSDs that meet strict criteria. The present study showed that large devices could be inserted through the puncture hole in the RV in a cat without major complications. However, careful consideration of strict, detailed criteria and adaptive methods is necessary.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
1. Tidholm, A., Ljungvall, I., Michal, J., Haggstrom, J., Hoglund, K. (2015). Congenital heart defects in cats:A retrospective study of 162 cats (1996-2013). J Vet Cardiol. 17, Suppl 1. S215-219. https://doi.org/10.1016/j.jvc.2014.09.004 PMid:26776580
2. Cote Kam, E., Meurs, K.M., Sleeper, M.M. (2011). Feline cardiology. (pp.85-100). Wiley-Blackwell. https://doi.org/10.1002/97811187ↂ2
3. Bomassi, E., Misbach, C., Tissier, R., Gouni, V., Trehiou-Sechi, E., et al. (2015). Signalment, clinical features, echocardiographic findings, and outcome of dogs and cats with ventricular septal defects:109 cases (1992-2013). J Am Vet Med Assoc. 247 (2):166-175. https://doi.org/10.2460/javma.247.2.166 PMid:26133216
4. Eyster, G.E., Whipple, R.D., Anderson, L.K., Evans, A.T., O'Handley, P. (1977). Pulmonary artery banding for ventricular septal defect in dogs and cats. J Am Vet Med Assoc. 170 (4):434-438. PMid:557030
5. Sheridan, J.P., Mann, P.G., Stock, J.E. (1971). Pulmonary artery banding in the cat:a case report. J Small Anim Pract. 12 (1):45-48. https://doi.org/10.1111/j.1748-5827.1971.tb05633.x PMid:5103104
6. Warden, H.E., Cohen, M., Read, R.C., Lillehei, C.W. (1954). Controlled cross circulation for open intracardiac surgery:physiologic studies and results of creation and closure of ventricular septal defects. J Thorac Surg. 28(3):331-341; PMid:13192880
7. Breznock, E.M., Hilwig, R.W., Vasko, J.S., Hamlin, R.L. (1970). Surgical correction of an interventricular septal defect in the dog. J Am Vet Med Assoc. 157 (10):1343-1353. PMid:5529824
8. Fujii, Y., Fukuda, T., Machida, N., Yamane, T., Wakao, Y. (2004). Transcatheter closure of congenital ventricular septal defects in 3 dogs with a detachable coil. J Vet Intern Med. 18(6):911-914. https://doi.org/10.1111/j.1939-1676.2004.tb02643.x PMid:15638280
9. Shimizu, M., Tanaka, T., Hirao, H., Kobayashi, M., Shimamura, S., et al. (2005). Percutaneous transcatheter coil embolization of a ventricular septal defect in a dog. J Am Vet Med Assoc. 226 (1):52-63, 69-72. https://doi.org/10.2460/javma.2005.226.69
10. Margiocco, M.L., Bulmer, B.J., Sisson, D.D. (2008). Percutaneous occlusion of a muscular ventricular septal defect with an Amplatzer muscular VSD occluder Amplatzer J Vet Cardiol 10(1):61-66. https://doi.org/10.1016/j.jvc.2008.01.001 PMid:184⇑9
11. Lock, J.E., Block, P.C., McKay, R.G., Baim, D.S., Keane, J.F. (1988). Transcatheter closure of ventricular septal defects. Circulation 78 (2):361-368. https://doi.org/10.1161/01.CIR.78.2.361 PMid:3396173
12. Uechi, M., Hirada, K., Mizukoshi, T., Mizuno, T., Mizuno, M., et al. (2011). Surgical closure of an atrial septal defect using cardiopulmonary bypass in a cat. Vet Surg. 40 (4):413-417. https://doi.org/10.1111/j.1532-950X.2011.00798.x PMid:21466564
13. Borenstein. N, Gouni, V., Behr, L., Trehiou-Sechi, E., Petit, A., et al. (2015). Surgical treatment of cor triatriatum sinister in a cat under cardiopulmonary bypass. Vet Surg. 44 (8):964-969. https://doi.org/10.1111/vsu.12403 PMid:26414173
14. Schneider, M., Hildebrandt, N. (2003). Transvenous embolization of the patent ductus arteriosus with detachable coils in 2 cats. J Vet Intern Med. 17 (3):349-353. https://doi.org/10.1111/j.1939-1676.2003.tb02460.x PMid:12774978
15. Saunders, A.B., Carlson, J.A., Nelson, D.A., Gordon, S.G., Miller, M.W. (2013). Hybrid technique for ventricular septal defect closure in a dog using an Amplatzer (R) Duct Occluder II. J Vet Cardiol. 15 (3):217-224. https://doi.org/10.1016/j.jvc.2013.06.003 PMid:23962683
16. Koneti, N.R., Sreeram, N., Penumatsa, R.R., Arramraj, S.K., Karunakar, V., et al. (2012). Transcatheter retrograde closure of perimembranous ventricular septal defects in children with the Amplatzer duct occluder II device. J Am Coll Cardiol. 60 (23):2421-2422. https://doi.org/10.1016/j.jacc.2012.08.1004 PMid:23141497
17. Zhou, D., Pan, W., Guan, L., Ge, J. (2012). Transcatheter closure of perimembranous and intracristal ventricular septal defects with the SHSMA occluder. Catheter Cardiovasc Interv. 79 (4):666-674. https://doi.org/10.1002/ccd.23344 PMid:22109986
© 2017 Uemura A. This is an open-access article publishedunder the terms of the Creative Commons Attribution License whichpermits unrestricted use, distribution, and reproduction in any medium,provided the original author and source are credited.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
Macedonian Veterinary Review. Volume 40, Issue 2, Pages 183-187, p-ISSN 1409-7621, e-ISSN 1857-7415, DOI: 10.1515/macvetrev-2017-0022, 2017