Mac Vet Rev 2018; 41 (2): 133 - 141
 10.2478/macvetrev-2018-0016
10.2478/macvetrev-2018-0016
Received: 14 September 2017
Received in revised form: 05 January 2018
Accepted: 22 January 2018
Available Online First: 31 May 2018
Published on: 15 October 2018
Keywords: ESBL-producing Escherichia coli, resistance profile, GUT colonization, PFGE- typing
Escherichia coli (E. coli) is one of the dominating species of bacteria living in the intestines of mammals, known as commensally gastrointestinal flora (1). The gastrointestinal tract (GUT) is a complex eco-system which includes approximately 800-1000 different bacterial species (2), and the GUT microbiome accounts for more than three million genes (3). The diversity of this bacterial eco – system is relatively poor in infancy, but later it reaches complexity and it stays relatively stable during life (4). The most dramatic disturbance of the ecological balance established between members of the commensally GUT flora and the human as a host is a result of antimicrobial administration (5, 6, 7).
ESBLs are enzymes that confer resistance to narrow – and expanded – spectrum cephalosporins, do not affect cephamycin and carbapenem compounds and are inhibited by clavulanic acid and other inhibitors of class A- β – lactamases (8, 9). Since their first publication (10), currently more than 220 TEM and 180 SHV enzyme varieties with ESBL characteristics have been detected (11). CTX – M is a recently described group of ESBL enzymes (12). These enzymes successfully hydrolyze cefotaxime but are less successful in hydrolyzing ceftazidime (the reason for their name). CTX – M are reported from different parts of the world and it seems that these are the most prevalent ESBL enzymes nowadays (13, 14).
In order to study the epidemiology of ESBL- E. coli, Pulsed-Field Gel Electrophoresis (PFGE) was used as a “gold standard” for genotyping. PFGE has a high reproducibility and discriminatory power to differentiate unrelated strains and also to demonstrate the relationship of organisms deriving from the same source. PFGE can be used for the comparison of large genomic DNA fragments after digestion with a restriction enzyme, while the usage of PFGE for genotyping of ESBL - E. coli is well established in the literature (15, 16).
To our best knowledge, this is the first study about relationships between respiratory tract colonization/infection with ESBLs – E. coli and GUT as endogen reservoir of these bacteria in infants with respiratory tract infections.
The study population consists of patients with respiratory tract infections hospitalized at the Institute for Respiratory Diseases in Children, in the period from November 2014 to June 2015. A total of 1,594 clinical samples of sputum or tracheal aspirates were investigated and 155 of them (9.7%) were culture positive for Enterobacteriaceae. In order to test the hypothesis for indigenous source of ESBL- E. coli colonizing the respiratory tract (RT) in infants, besides the sputum specimens, 40 rectal samples (rectal swabs) were taken from patients (study group) for further microbiological analyses. Data collected from medical documentation such as: gender, age, date of admission to hospital, date of sampling sputum or tracheal aspiration for microbiological investigation, diagnosis, wards where the patients were admitted, antibacterial treatment in ambulatory settings before hospitalization, antibacterial treatment during hospitalization, and previous hospitalizations (in the last four months) were analyzed in order to determine some of the risk factors for colonization of RT with ESBL – E. coli. The control group (n=15), were healthy children under the age of one. Rectal swabs were taken in order to isolate E. coli – strains. All participants (parent or legal guardian) in the study group or in the control group gave written informed consent. This study was approved by the Ethical Commission at the Medical Faculty, University Ss Cyril and Methodius, Skopje (03-1055/5).
Isolates from the respiratory tract specimens were obtained during routine laboratory work and in order to isolate and identify bacteria, standard microbiological procedures were used. The following nutritive plates were utilized: blood agar plate (Oxoid Ltd, Basingstoke, UK), chromogenic agar plate – UTI (Oxoid Ltd, Basingstoke, UK), and chromogenic selective medium for ESBL screening - ChromoID ESBL agar (bioMerieux, France).
Rectal swabs were cultured on two plates: blood agar plates and Chromo ID-ESBL. After overnight incubation at 37°C, the growth of purple colonies on the Chromo ID-ESBL indicated the presence of ESBL-E. coli. In order to select colonies with similar morphology to those isolated from the respiratory tract, 2-3 colonies with such morphology were picked up from the blood agar plates, and subcultivated on Chromo ID-ESBL. The isolates with color indicating E. coli were included for further processing.
Only one pair of isolates (each pair contains ESBL-producing E. coli strains detected from sputum and rectal swab from the same patient) per patient were included for further analyzing.
Antimicrobial susceptibility was determined by the disk diffusion method using European Antimicrobial Susceptibility Testing (EUCAST) – specified procedures, and interpretative criteria (17). Agents tested included amoxicillin/clavulanic acid, cefotaxime, ceftazidime, cefoxitin, imipenem, ciprofloxacin, trimethoprim-sulfamethoxazole, amikacin, gentamicin. Strains which were resistant towards some of the third generation cephalosporins were selected as suspect ESBL producers, and double- disk synergy test (DDST) was used as phenotypic confirmatory test for ESBL detection (18). This test is based on synergy acting between third generation cephalosporins and clavulanic acid. The susceptibility disk containing amoxicillin-clavulanate, was placed in proximity to disks containing ceftazidime (CAZ) and cefotaxime (CTX). Enhancement of the zone of inhibition of the CAZ and CTX caused by the synergy of the clavulanate in the amoxicillin-clavulanate - disk, indicates the presence of ESBL enzymes.
In order to analyze the relatedness between ESBL – E. coli, 25 pairs with identical resistance profile from the study group and 15 isolates from the control group, underwent pulsed-field gel electrophoresis (PFGE) analysis of Xbal-restricted total DNA (n=65). The procedure was performed according to the PulseNet protocol (19), with minor modification. A turbidimeter was used for cell suspension measurement between 1.8 to 2.0 MacFarland (while turbidimeter is not recommend in the original method). Cell suspension volume used for plug preparation was reduced to 200 µL (instead of 400 µL). Elaboration of the band patterns was done by using computer FPQuest software version 5.10 (BIORAD, USA). Dendrogram was generated by the unweighted pair group method using arithmetic average (UPGMA), using Dice coefficient with optimization and tolerance set at 1%. The interpretation of the PFGE followed the recommendation of the EFSA standard operating procedure for PFGE profiles interpretation (20). At least one band difference was chosen as a limit to consider two PFGE profiles different, as recommended by Barrett et al. (21). We used a down limit for band interpretation at 33kbp as recommended for Salmonella by Peters et al. (22).
Of a total of 155 isolated Enterobacteriaceae, 78.1% (121/155) were confirmed as E. coli of which 79.3% (96/121) were found as ESBL – producers. Antimicrobial susceptibility testing of ESBL - E. coli strains (n=96), demonstrated a 100% resistance to 3rd generation cephalosprins (cefotaxime, ceftazidime), and no resistance was observed to imipenem. The other tested antimicrobials were: gentamicin, amikacin, ciprofloxacin, amoxicillin-clavulanic acid, trimethoprim-sulfamethoxazole and the resistance rates were 83.3%, 9.4%, 17.7%, 33.3 % and 4.2%, respectively.
In the study group, ESBL- E. coli was isolated from all (n=40) cultivated rectal specimens. The comparison of the antimicrobial susceptibility patterns of the paired strains, where each pair contains ESBL-producing E. coli detected from sputum (s) and rectal swab (r) from the same patient, demonstrated identical resistance profile in 90% (36/40).
33.3% (5/15) of confirmed E. coli strains from the control group were found to be ESBL – producers.
65 strains of E. coli, out of which 25 pairs with identical resistance profile from the study group and 15 isolates from the control group, were PFGE typed using Xbal digestion.
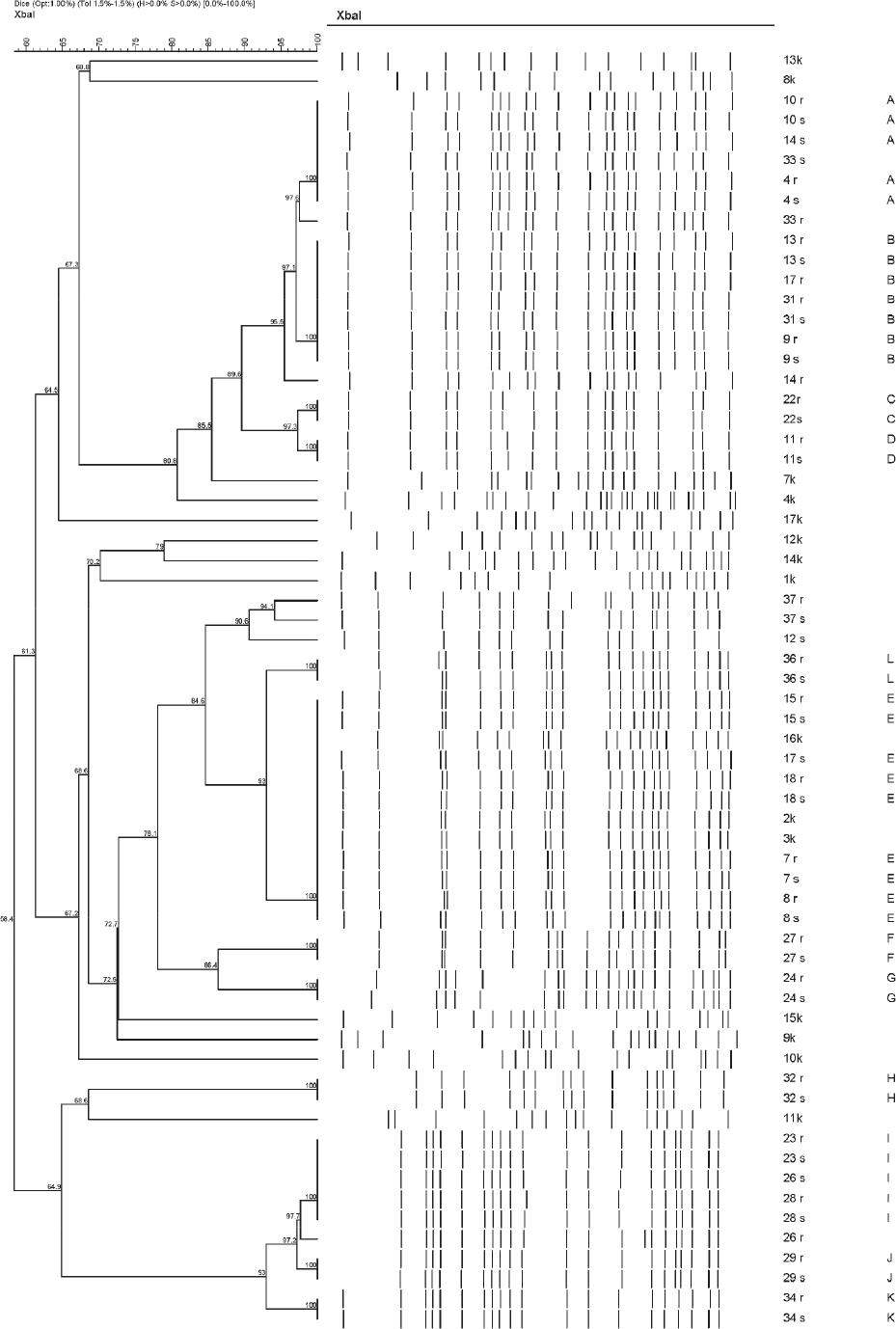
PFGE pulsotypes grouped indistinguishable profiles according to interpretation criteria. They were defined by a letter code from A to L (Fig.1). One pair (12s and 12r) cannot be compared because of technical issues (PFGE-bands were not obtained for 12r). 19 out of the 24 compared pairs belonged by pair to the same pulsotype. Two compared pairs (26s and 26r, 33s and 33r) showed only one band difference.
Figure 1. Dendogram (UPMGA clustering based on Dice correlation coefficient, Opt 1,0 %, Tol 1,5 %) of Escherichia coli Xbal PFGE patterns. The same number of the strains from the study group – indicates strains obtained from the same patient; s (strain obtained from sputum); r (strain obtained from rectal sample); k- strain from the control group
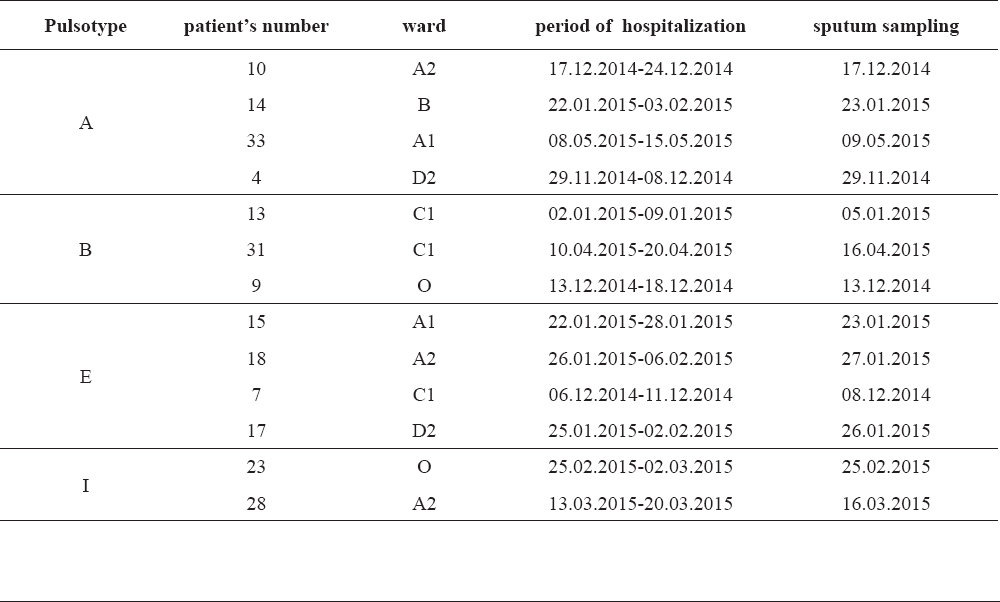
The wards where the patients were admitted, the time of sputum sampling and the period of hospitalization were analyzed in order to trace the location of the patients through their hospital stay. This data, for patients with ESBL- E. coli isolates grouped in the same pulsotypes, is given in Table 1.
Table 1. Wards and period of hospitalization of the patients with isolated ESBL -E. coli strains grouped in the same pulsotypes
In the control group (k) a genetic diversity was present (Fig.2), but three of the strains (16k, 2k and 3k) which were ESBL-producers, belong to same pulsotype - pulsotype E (Fig.1).
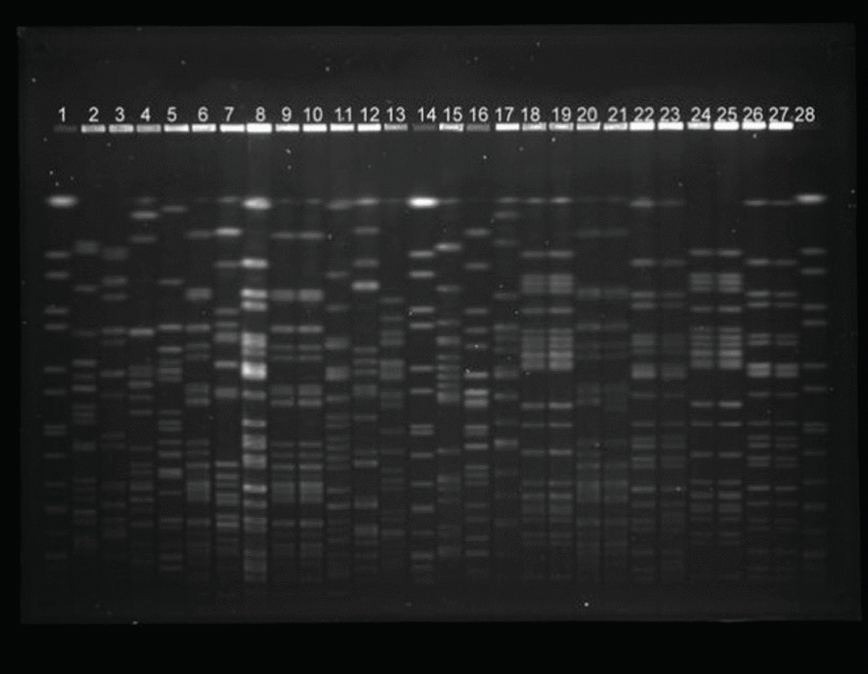
Figure 2. Xbal restriction PFGE profile of 25 Escherichia coli isolates. At position 1, 14 and 28 is Salmonella braenderup H9812(Sb) as a marker. At the other positions are the following isolates: 2-1k, 3-8k, 4-9k, 5-17k, 6-16k, 7-1k, 8-4k, 9-3k, 10-2k, 11-7k,12-10k, 13-14k, 15-15k, 16-12k, 17-13k, 18-34s, 19-34r, 20-37s, 21-37r, 22-33s, 23-33r, 24-29s, 25-29r, 26-31s, 27-31r; k-control group; s-sputum; r-rectum
According to data collected from the medical documents, the average age of the study group was 6.8 months (from 2mth to 13mth). All patients in the study group were treated with parenteral third generation cephalosporins and in 60% (24/40) antibiotic treatment was initiated in ambulatory settings before hospitalization. Previous hospitalization (in the last four months) was present in 52.5% (21/40) of the patients.
Until the end of the 1990s, ESBLs – isolates were mainly associated with nosocomial outbreaks and the prevalence of ESBL producers was higher among Klebsiella pneumoniae than among E. coliisolates (23). This situation has changed dramatically, and the most ESBL-producing isolates are now E. coli mainly associated with community acquired infections (24, 25). Despite extensive studies of ESBL- producing organisms in adult patients, there is a lack of information about the epidemiology and spread of ESBL - organisms in pediatric population (26).
Apart from antibiotic selective pressure (previous hospitalization was present in 52.5% of the patients in the study group and in 60% of the patients antibiotic treatment was initiated in ambulatory settings before hospitalization), in our study the risk factor for colonization/infection of the respiratory tract with ESBL- producing E. coli strains was the young age of the patients (under the age of one). Acid gastric content is a huge barrier for bacteria, but according to Mitchella et al. (27), gastric content in infancy has different biochemical characteristics, mainly because of the milk feeding. Milk is the basic food for infants and it has nearly neutral pH and significantly specified buffer capacity. Because of that for a long period of time, the gastric content in infants has pH>4 (27). Besides the pH values of the gastric content, the length of the esophagus, the immaturity of the gastro-esophageal sphincter and the horizontal (supine) position are possible risk factors for bacterial translocation in infants.
There is research on adult patients, especially hospitalized in intensive care units (ICU), which connect worsening of the condition because of aspiration, due to supine position (28, 29). In the work of Drakulovic et al. (30) and Pingleton et al. (31), infections in patients in a supine position were strongly associated with enteral nutrition, mainly because of an increased risk of aspiration of gastric content. 22.5% (9/40) of the infants in our study group were suspected for reflux disease, as it was noted in the medical records.
According to data collected from the medical documents, most of the patients had signs of low respiratory tract infection at the time of admission to hospital, and no one satisfied the criteria for hospital acquired pneumonia (32). Although some isolates obtained from different patients were genetically indistinguishable, there was a lack of obvious transmission chain. The patients with closely related strains were admitted at different wards and if they derived from the same ward, hospitalization was during different periods of time (Table 1). Some strains which belong to different groups have identical antimicrobial susceptibility patterns. This indicates the necessity of molecular- typing - methods for tracing of hospital infections, because the phenotypic methods for this purpose are not sufficient.
On the other hand, three strains obtained from the control group of healthy children, belong to pulsotype E. It seems that it may not be unusual for two patients to be admitted to the same hospital, to the same ward, already colonized/infected with highly related strains. This consideration corresponds to the observation made by Prosperi et al. (33).
Tschudin-Sutter et al. (34) stated that there is a low transmission rate of E. coli, including ESBL – producers, which contributes to the hypothesis for endogen source of the strains. Mainly, this is because ESBL-producing E. coli in contrast to multidrug-resistant gram-positive organisms such as methicillin - resistant Staphylococus aureus (MRSA) and vancomycin - resistant Enterococci (VRE), do not survive either on dry surfaces in the environment nor on the human skin (35, 36).
On the other hand, 19 out of the 24 compared pairs (each pair contains ESBL-producing E. coli strains detected from the sputum and the rectal swap from the same patient), belong by pair to the same pulsotype. This suggests that in most cases, a resistant clone becomes dominant in the eco - system of the GUT and this clone successfully colonizes the respiratory tract in this particular infant. In addition, two pairs (26s and 26r, 33s and 33r) did not belong to the same pulsotype but showed closely related profiles, with only one single band of difference. The relatedness between these strains remained to be demonstrated.
According to the results from the PFGE comparison of all isolates, it can be concluded that ESBL-producing E. coli isolated from the respiratory tract were indigenous to the gastrointestinal tract flora and the GUT is their main reservoir. The use of antibiotics is already a well-established risk factor for appearance of ESBL - producing strains. Lack of obvious evidence for hospital transmission of bacteria, as well as a high percentage of digestive colonization in the control group suggest increased risk for influx of ESBL- E. coli from the community to the hospitals. Small age is a risk factor for translocation of bacteria, enabling the respiratory tract colonization in infants with respiratory tract infections.
©2018 Popova G. This is an open-access article published under the terms of the Creative Commons Attribution License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The authors acknowledge the medical staff at the Institute for Respiratory Diseases in Children-Skopje for providing medical records for the patients in the study group. Special thanks go to Dr. Sanja Cileska for her help in collecting biological specimens from the participants in the control group.
The authors declared that they have no potential conflict of interest with respect to the authorship and/or publication of this article.
Macedonian Veterinary Review. Volume 41, Issue 2, Pages 133-141, p-ISSN 1409-7621, e-ISSN 1857-7415, DOI: 10.2478/macvetrev-2018-0016, 2018