The retrospective study investigated hematological and biochemical differences in dogs with neoplastic splenic disease (NSD), comparing malignant versus non-malignant, as well as malignant lymphoid versus malignant non-lymphoid tumors. The research included 20 dogs with splenic disease admitted at the University Veterinary Hospital in Skopje within three years. Each dog underwent clinical examination, abdominal ultrasound, blood, serum, and cytology analysis. Based on cytological findings, dogs were divided into two groups: malignant (M, n=14) and benign (B, n=6) spleen disease. The M group was further divided into malignant lymphoid (ML, n=6) and malignant non-lymphoid (MNL, n=8) subgroups. Data (mean±SEM) was analyzed with Kruskal-Wallis and Mann-Whitney U Test with significance levels set at p<0.05. The M group had significantly higher values than B group for white blood cell (32.08±9.29 and 7.37±0.96x109/L, respectively), monocyte (2.89±1.09 and 0.64±0.12x109/L, respectively), neutrophil counts (17.46±3.80 and 5.39±0.88x109/L, respectively), alanine aminotransferase (82.52±12.49 and 36.89±4.14 IU/L, respectively), and alkaline phosphatase levels (279.16±62.06 and 111.80±15.40 IU/L, respectively). Within the M group, ML subgroup had significantly higher values than MNL for white blood cell (62.80±19.65 and 15.02±3.03x109/L, respectively) and neutrophil counts (29.02±7.86 and 11.04±2.22x109/L, respectively), but lower for alkaline phosphatase (252.80±56.02 and 293.80±93.76 U/L, respectively). Ultrasonographic findings of heterogenous hypoechoic nodules (‘leopard’ pattern), pleomorphic lymphoblasts infiltration, and elevated leucocytes, neutrophils, monocytes, alanine transaminase, and alkaline phosphatase, may aid in differentiating malignant from benign NSD in dogs. Additional to the ultrasonographic and cytology findings, elevated leucocytes, neutrophils, and alkaline phosphatase effectively differentiate lymphoid from non-lymphoid NSD in dogs.
The spleen is a significant part of the lymphatic system in dogs related with lymphopoiesis, erythrocyte and platelet storage, phagocytosis of old and damaged erythrocytes, blood filtration, extramedullary hematopoiesis, and iron metabolism (
1). Neoplastic spleen diseases (NSD) are a significant contributing factor for the morbidity and mortality in middle-aged and older dogs, which may vary from mild, chronic, nonspecific clinical form, to peracute clinical form resulting in fatal hemoabdomen (
2). The hematological and biochemical findings may be quite variable. Anemia may occur frequently during NSD, but its association with neoplasia is often non specific and with uncertain diagnostic reliability (
3). Anemia may occur during various chronic diseases, bone marrow dysfunctions, hemolysis due to lymphoproliferative disease, infection, or immune-mediated diseases (
2). Thrombocytopenia is another common hematological finding during NSD, and can also be related with immune-mediated paraneoplastic syndrome (
4), lymphoproliferative process, sepsis, or ehrlichiosis (
2). NSD may result in elevated alkaline phosphatase, which is the most frequently observed biochemical change in dogs with neoplasia (
5).
Ultrasonographic finding of splenomegaly is commonly observed during NSD and is highly correlated with neoplastic changes (
6). Splenomegaly can be generalized or localized in the form of a splenic mass which may have malignant or benign characteristics. Some of the most common localized benign changes are splenic hematoma, nodular hyperplasia, abscess, and hemangioma. Inflammatory, hyperplastic, and congestive splenomegaly are most commonly related with generalized benign abnormalities of the spleen. Generalized spleen changes are commonly related to malignant NSDs, such as infiltrative splenomegaly where the splenic tissue is most commonly infiltrated by malignant neoplastic cells (
7). The most common malignant NSD is lymphoma (
8) with prevalence of 20-100 in 100,000 dogs (
9). Splenic hemangiosarcoma is another commonly observed malignant NSD in dogs (
8) composed of immature endothelial cells, vascular spaces, small clefts, and cavernous channels. These structures contain a variable amount of blood and can sometimes initiate formation of thrombotic masses. The newly formed vessels by the neoplasm are fragile and can easily rupture, resulting in hemorrhage (
7).
The high variability of clinical, hematological, and biochemical findings in dog NSDs renders these parameters to be non-specific and of low diagnostic importance. However, the current study hypothesized that there may be higher specificity and difference between the benign, malignant lymphoid, and malignant non-lymphoid NSDs for the hematological and biochemical parameters. The aim of the current study was to compare the hematological and biochemical parameters between malignant and benign NSDs confirmed by ultrasonographic and cytology diagnosis, and more specifically, to elucidate the differences among the malignant lymphoid, non-lymphoid, and benign NSDs in dogs.
MATERIAL AND METHODSThe study included 20 dogs with splenic-related disorders of various age, sex, and breed admitted at the University Veterinary Hospital at the Faculty of Veterinary Medicine-Skopje, Ss. Cyril and Methodius University in Skopje over a period of 3 years. A diverse range of dog breeds was included: 4 Labrador Retrievers, 3 Golden Retrievers, 3 German Shepherds, 2 Shar-Peis, 1 Corgi, 1 Maltese, 1 French Bulldog, 2 Boxers, 1 Cocker Spaniel, 1 Pug, and 1 Staffordshire Terrier. The patients were between 5 and 11 years of age. Twelve of the patients were male and eight were female. All animals included in this study underwent standard clinical and diagnostic procedures with respect to animal welfare. Clinical records were obtained and used for research purposes with the owner’s consent. Under these circumstances, no Ethical Approval was deemed necessary since the procedures were routine and the data was used for scientific purposes with consent of the owners. Upon admission, the dogs were subjected to clinical examination, abdominal ultrasound, complete blood count, serum, and cytology analysis, routinely performed as part of the diagnostic procedures.
The ultrasound examination was performed with an Esaote MyLab30Gold ultrasound machine (Esaote, Italy) or Vetus 8 (Myndray, China) with a microconvex probe. Abdominal retrocostal or intercostal left approach was used on the left caudal thoracic wall. Size, shape, echogenicity, and echotexture of the spleen were determined for each dog. Splenic formations were noted and characterized.
Blood samples were taken from the cephalic vein in EDTA vacutainers and were analyzed on a veterinary hematology analyzer Exigo (Boule, Sweden). The following hematological parameters with their respective reference ranges were obtained: erythrocyte blood count (RBC-5.50-8.50x10
12/L), packed cell volume (PCV-47-55%), hemoglobin (HGB-12-18 g/dL), platelets (PLT-200-500x10
9/L), white blood cells count (WBC-6-17x10
9/L), lymphocytes (LYM-1.2-5.0x10
9/L), monocytes (MON-0.3-1.5x10
9/L), and neutrophils (NEU-3.5-12.0x10
9/L).
Blood samples for biochemical analysis were collected in a vacutainer without anticoagulant. The sera of these blood samples were analyzed on an automatic biochemical spectrophotometer ChemWell 2910 (AwarenessTechnology INC, USA), according to the manufacturer instructions (Human, Germany). The following biochemical parameters with their respective reference ranges were obtained: alanine transaminase (ALT-8.2 57.3 IU/L), aspartate aminotransferase (AST-8.9-48.5 IU/L), alkaline phosphatase (AP-10.6-100.7 IU/L), total proteins (TP-54.1-75.2 g/L), albumins (ALB-25.8-44.7 g/L), creatinine (CRT-44.3-138.4 umol/L), and urea (UREA 3.14-9.25 mmol/L). Reference values for hematology and biochemistry were obtained from Merck Veterinary manual.
The cytology samples were taken by using ultrasound guidance with a 21G needle with the ‘fine needle aspiration’ method described elsewhere (
10). Briefly, the patients were placed in lateral recumbency and the spleen was positioned towards echogenic area where it could be safely punctured avoiding lesions and bleeding. After shaving, the skin was aseptically and antiseptically treated with 70% ethanol solution and 10% iodine povidone. Percutaneous punction was performed with needle guided by an ultrasound probe. The collected material was smeared between two microscopic slides and was stained with Diff Quick (Merck, Germany) (
10). The slides were analyzed on binocular microscope (Leica, Germany) at 40x and 100x magnification. Cell morphology, cytoplasmatic and nuclear structure, number of cells, and extracellular matrix were evaluated on the microscope slides for each sample.
Following the clinical, ultrasonographic, and cytology findings, the dogs were divided in two major groups, malignant - M (n=14) and benign - B (n=6) splenic disease. The M group was additionally divided into malignant lymphoid - ML (n=6) and malignant non-lymphoid - MNL (n=8) splenic disease subgroups.
The data (mean±standard deviation) were compared with Kruskal-Wallis and Mann-Whitney U Test with effect size of 0.25, error probability of 0.05, total sample size of 20, number of groups 2 (Statistica v8, StatSoft Inc.). The power of the tests was estimated with G*Power (v. 3.1.9.2, University of Kiel, Germany). The analysis for Mann-Whitney test was employed with power of 0.16 (df=17), whereas for Kruskal-Wallis, it was 0.14 (df=17). Significant differences were considered at p<0.05.
RESULTSUltrasonographic findings
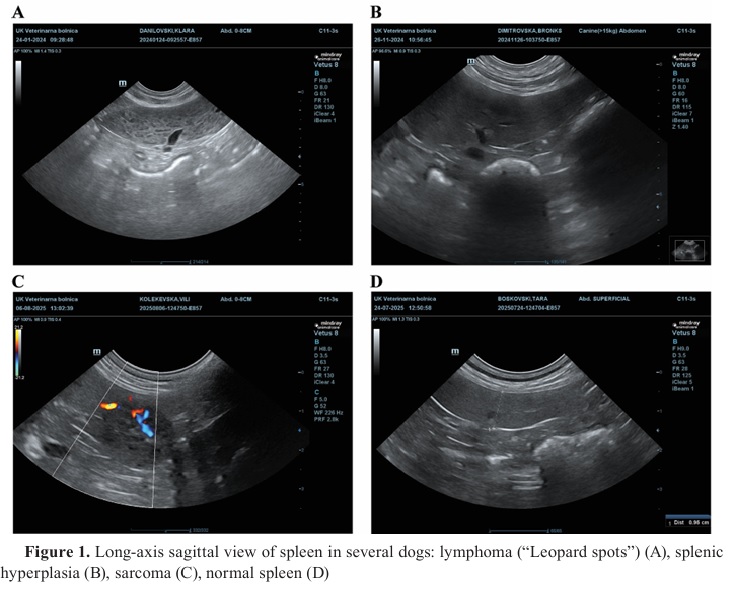
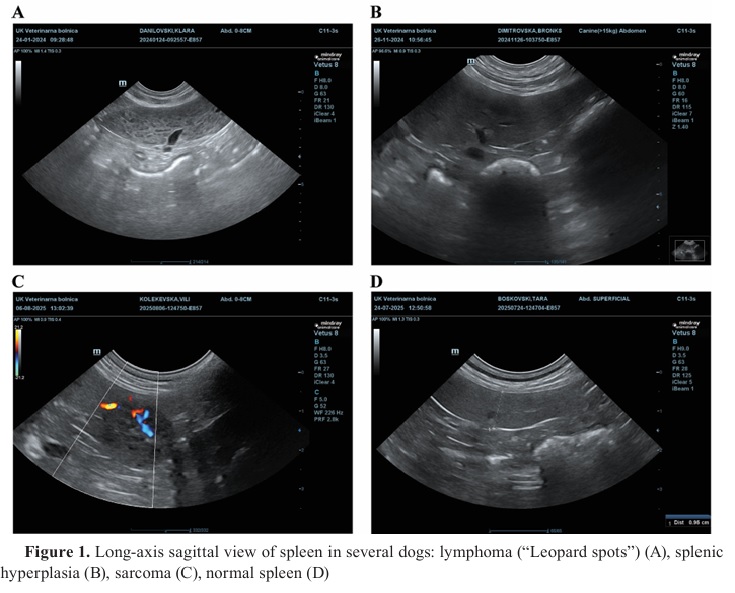
Lymphoid malignancies (lymphoma) (n=6) were mostly with heterogeneous echotexture visualized as multiple hypo-echoic nodules with a leopard spots appearance of the spleen (n=5) (
Fig. 1), and as single heterogeneous focal mass (n=1). Non-lymphoid malignancies (sarcomas) (n=8) appeared mostly as single or multiple hypo-echoic heterogenous masses with variable size (0.3-5.0 cm).
The larger tumor lesions had anechogenic cavity formations with irregular shapes localized inside the neoplastic mass. Benign spleen changes (n=6) were mostly manifested with splenomegaly and inhomogeneous splenic echotexture.
 Cytology findings
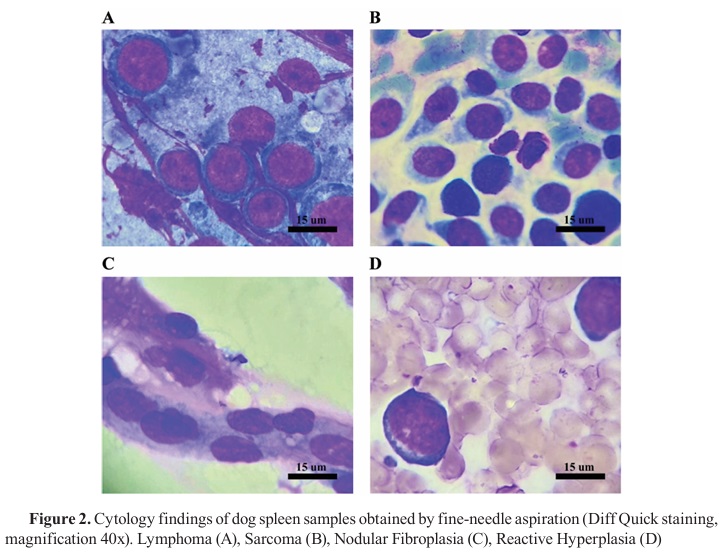
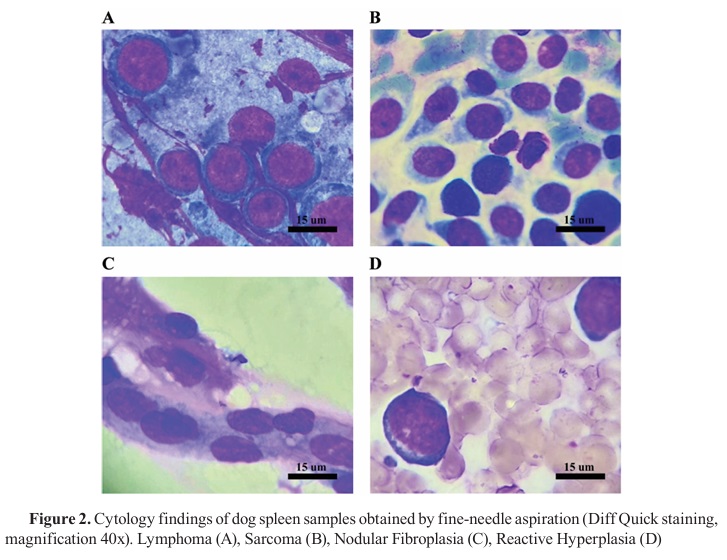
Cytology findingsMicroscopy evaluation of spleen cell cytology revealed various cellular and extra cellular matrix characteristics. Benign spleen lesions had typical lymphoid cell population composed of small mature lymphocytes, reactive lymphocytes, intact neutrophils, monocytes, fibrocytes, and erythrocytes characterized by normochromic erythroisocytosis. Malignant spleen lesions had numerous pleomorphic atypical cells with immature characteristics. Lymphoblasts were predominant cell population in the malignant lymphoid neoplasia, with round shape and immature cellular and nuclear morphology characteristics (anisocytosis and anisonucleosis).
Hemangiosarcoma/hemangiopericytoma, or soft tissue sarcoma, had pleomorphic cell cytology of different cell lines. Individual mesenchymal cells were with indistinct cytoplasmatic borders, pale bluish cytoplasm with discrete vacuolization, oval or elongated anisokariotic nucleus with coarse chromatin and prominent metachromatic nucleolus. Histiocytic sarcoma was characterized with discrete round cells with characteristic cellular, cytoplasmatic, and nuclear changes with mitotic formations (
Fig. 2).
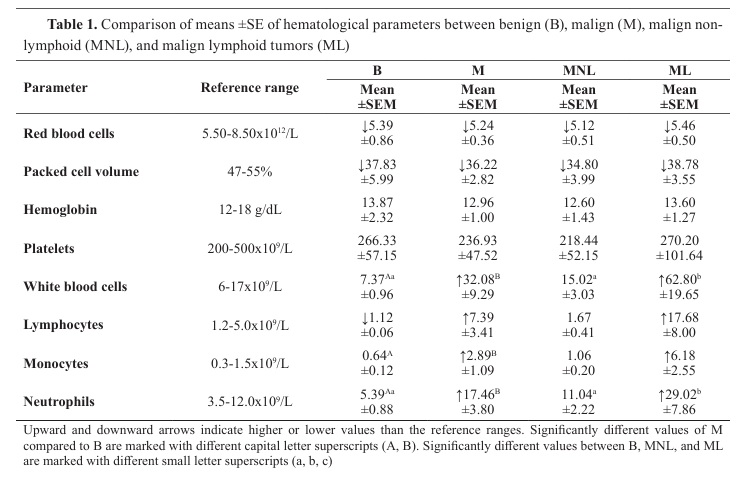
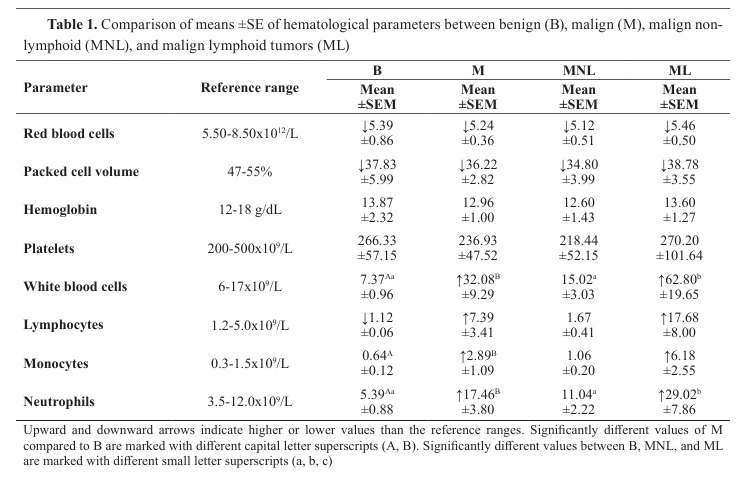
Hematological and biochemistry findingsRBC and PCV were decreased bellow the lower reference value in all groups, but they did not differ significantly. HGB and PLT were in the reference ranges for all groups and did not differ significantly. WBC were in the reference range for B (7.37±0.96x10
9/L) and MNL (15.02±3.03x10
9/L, but were significantly higher for M (32.08±9.29x10
9/L) and ML (62.80±19.65x10
9/L). ML had significantly higher WBC compared to B and MNL (15.02±3.03x10
9/L). MNL had significantly lower WBC compared to ML. The LYM were non significantly different among the groups due to the high variances, despite the high numerical differences. M (7.39±3.41x10
9/L) and ML (17.68±8.00x10
9/L) had higher LYM than the reference range, whereas B had small negative deviation from the lower reference value. M was had non-significantly higher LYM compared to B (1.12±0.06x10
9/L). MON were above the reference range in the M group (2.89±1.09x10
9/L) mostly contributed by the ML group (6.18±2.55x10
9/L). MON in B (0.64±0.12x10
9/L) and MNL (1.06±0.20x10
9/L) were in the reference range. The M group had significantly higher MON compared to B, whereas no significant differences were observed between MNL and ML. The NEU were above the reference range in the M group (17.46±3.80x10
9/L) mostly contributed by the ML group (29.02±7.86x10
9/L). NEU were significantly higher in M compared to B (5.39±0.88x10
9/L). Significant difference in NEU was observed in ML compared to B, as well as between ML and MNL (11.04±2.22x10
9/L). No significant difference was observed in NEU between MNL and B. More detailed data for the hematological parameters can be found in
Table 1.
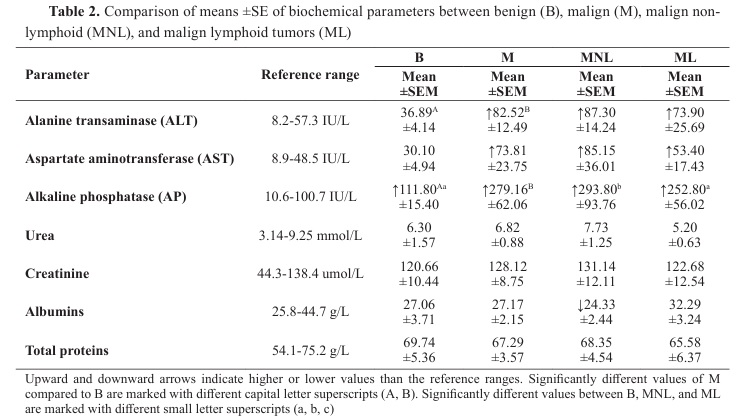
The urea, creatinine, and total proteins were in the reference range for all groups and they were non-significantly different. The albumins were non-significantly different among the groups and were in the reference range for all groups with exception of MNL (24.33±2.44 g/L) which was below the lower reference value. AST value in M (73.81±23.75 U/L) was above the reference range mostly due to MNL group (85.15±36.01 IU/L).
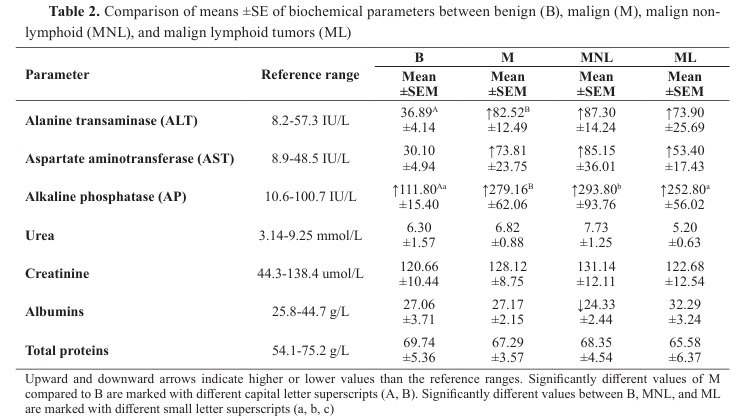
The AST in ML (53.40±17.43 IU/L) was above the reference range but had little contribution to M. However, there was no significant difference in the AST level between the groups. ALT had higher than the reference range values in M (82.52±12.49 IU/L), and more specifically in MNL (87.30±14.24 IU/L) and ML (73.90±25.69 IU/L). ALT was within the reference range in B (36.89±4.14 IU/L). Significant differences were observed between B and M, however, no significant differences were found between MNL and ML, neither between these two groups and B. AP level was above the reference range in all groups. M group (279.16±62.06 IU/L) had significantly higher AP value compared to B (111.80±15.40 IU/L). MNL (293.80±93.76 IU/L) had significantly higher AP value compared to B, but non-significantly higher compared to ML (252.80±56.02 IU/L). ML was non-significantly different compared to B. More detailed data for the biochemical parameters can be found in
Table 2.
DISCUSSIONLymphoma is a common spleen malignancy in dogs which can be observed on ultrasound as a solitary formation or as multiple hypo-echoic nodules with a “leopard-spot” pattern. This ultrasonographic finding was the most frequently observed in this study. Unlike lymphoma, nonlymphoid spleen tumors (e.g., sarcomas) appeared with or without splenomegaly with a poorly circumscribed, inhomogeneous mass of variable echogenicity (
2, 11). Although, ultrasonography is a highly sensitive tool for detecting focal spleen parenchymal abnormalities in dogs, it cannot be reliably used for differentiating specific diseases. Hence, distinguishing benign from malignant nodules by their ultrasonographic appearance is challenging, and needs to be confirmed by cytology.
Fine needle aspiration and Tru-cut needle biopsy are routinely performed to help distinguish benign from malignant lesions (
12). Cytology can be considered as a more reliable diagnostic tool which can help in determining the treatment approach (
13, 14, 15). The aspirated samples are analyzed by its cytology features, cell number and appearance, as well as by its extracellular matrix morphology. Cytology findings for hemangiosarcoma samples in the current study showed excessive blood infiltration (hemocontamination), immature mesenchymal cells, which according to its cellular and nuclear morphology, were deemed as atypia (
16). Cytology samples of spleen lymphoma are characterized by big round cells, especially lymphoblasts with anisocytosis and anisokariosis, with dark bluish scant cytoplasm and prominent nucleoli with rough chromatin content (
17). Benign spleen lesions with homogeneous echogenicity have uniform and typical cellular population of erythrocytes, small and reactive lymphocytes, monocytes, histocytes, macrophages, reticulocytes, and plasma cells (
18).
The current study hypothesized that NSD cases confirmed by cytology and ultrasonography can be correlated with biochemical and hematological indices. Additionally, the study hypothesized that these indices could potentially differentiate between malignant lymphoid from malignant non lymphoid NSD cases.
The observed hematological findings indicated on mild anemia with no significant differences in RBC between the benign and malignant groups. Usually, spleen lesions are concomitant with microangiopathies. Erythrocytes with poikilocytosis that pass through the altered vascular endothelium can be damaged or aggregated in the intercellular spaces of the red pulp. The occurrence of hypochromic anemia, erythrocyte sequestration, schistocytes, other types of altered erythrocyte morphologies, and hemophagocytic syndrome, could be considered as a predictive pattern of malignant metaplasia from nonlymphoid neoplasia (
14). The observed RBC values in the current study could also be related with а non-specific systemic reaction, and hence, they might not be directly associated with NSD. Several studies reported that dogs with anemia have lower survival rate than those without anemia. It has also been reported that malignant splenic disease and presence of hemoperitoneum have a negative association with the survival time (
15).
Similarly, packed cell volume and hemoglobin concentration were non-significantly different between the benign and malignant subgroups (MNL, ML), and could not be directly associated with NSD. However, it has been reported that anemia and nucleated red blood cells are associated with malignant tumors in dogs with splenomegaly (
15). The non-significant differences in platelet counts between the groups and their normal reference ranges was expected finding because the dogs included in the study were selected for biopsy. Additionally, the small size of the malignant formations in the ML group, without systemic infections, platelet degradation, adhesion, activation, and aggregation in the spleen blood vessels or connective tissue, could be contributing factor to the non-observable platelet changes. However, some other authors have reported an association between hemolymphatic disorders and cytologic alterations in the spleen (
17). Thrombocytopenia can be detected if there is a direct cytotoxic, antibody, and cytokine-mediated effect which can lead to enhanced destruction of platelets. Platelets also play a key role in cancer progression, contributing to tumor-associated inflammation. Therefore, platelets-to-lymphocyte ratio (PLR) may have more significant clinical role in distinguishing malignant from benign splenic lesions, though further validation is needed (
19).
The significantly higher leucocyte count in the malignant groups could be considered as an expected finding due to the immunological or systemic inflammatory response. Malignant diseases in spleen causes increased WBC as a result of chronic inflammation which is accompanied by release of interleukins (IL-1, IL-6, TNF-α), ischemic and necrotic changes of the malignant cells, immunological response, pain, stress, or secondary bacterial growth. The role of circulating lymphocytes remains complex, as both tumor suppressing and tumor-promoting mechanisms are involved (
20, 21, 22, 23). While CD8+ cytotoxic T lymphocytes contribute to tumor destruction, CD4+ T lymphocytes can support tumor progression through immune modulation. Therefore, the impact of lymphocytes on tumor dynamics can vary significantly (
19). The lymphoproliferative malignant neoplasia in the spleen was evident in the ML group which had significantly higher and above the reference range value of WBC compared to MNL with normal finding. Similarly, the lymphocyte count was 6-7-fold higher in the malignant groups compared to the benign group with 10-11-fold higher values in the ML compared to the MNL group. However, due to the high variability in the ML and low number of dogs, these differences were not significant. Nevertheless, circulating blood cells, such as neutrophils, lymphocytes, monocytes, erythrocytes, and platelets, have been used in human medicine as prognostic markers in various neoplasms (
19). The observed difference between the malignant groups was in line with the current scientific knowledge. Extramedullary lymphopoiesis with uncontrolled proliferation results in a release of morphologically immature and neoplastic lymphoblast cells (
17). Monocyte count finding was compliant with the WBC and LYM. The malignant groups had 4-5-fold higher MON values compared to the benign group. The ML group had 5-6-fold higher values compared to the MNL, which had normal values. However, these differences were non-significantly different due to the same reasons as explained earlier. Neutrophil count was significantly higher in the malignant groups compared to the benign group, with almost three-fold higher values. This difference was attributed due to the significantly higher values of the ML compared to the MNL group. The latter had normal, in reference range NEU values. Neutrophils facilitate tumor progression by promoting angiogenesis, immune suppression, attachment of circulating tumor cells to the endothelium. Spleen lymphoproliferative cells have antigenic properties which trigger non infectious inflammatory response with production and secretion of chemokines, integrins, and other factors. This can lead to an increased production and release of neutrophil, monocyte, and lymphocyte cells which was confirmed in the current study. The role of circulating lymphocytes remains complex, as both tumor-suppressing and tumor-promoting mechanisms are involved (
19).
Total protein concentration, urea, and creatinine were not changed beyond the upper and lower reference ranges nor they were significantly different between the groups. This was expected as the spleen is not directly associated with the protein metabolism and renal perfusion. Similar finding was reported even in the terminal stage of the disease (
24). Renal function was not associated with NSD. However, albumin fraction was below the reference range in the MNL, but there was no significant difference between the groups. It could be associated with higher catabolic activity of the non-lymphoid malignant cells. Systemic inflammation response is more expressed in MNL. The synthesis of proinflammatory cytokines inhibits albumin production in the hepatocytes; therefore, they are in lower concentration during the acute phase. Protein-losing syndrome and lack of albumin precursors are common in MNL. Conversely, ML is focal malignant proliferation without triggering severe systemic inflammatory response, so serum concentration of albumins remains in reference ranges. The findings of the current study are consistent with similar studies (
25).
The malignant group had twofold significantly higher value of ALT compared to the benign group, but no significant differences were observed between MNL and ML. Oliveira et al. (
26) reported increased serum levels of ALT, AST, and hypoalbuminemia as the most frequent biochemical alterations in female dogs with mammary neoplasms. The higher release of ALT from the hepatocytes could be an indication of a compressive effect of the neoplastic masses from the spleen on the liver. Similar findings have been reported by other authors (
24, 26).
AST had 2.45-fold higher value in the malignant compared to the benign group, however, even though it was markedly higher in the MNL, no significant differences were observed between either group. Since this enzyme is associated with tissue necrotic alterations, these findings were expected. Additionally, the higher values may be related with muscle tissue alterations induced by neoplasia in the abdominal muscles, elevated catabolism, as well as metastasis. The non-significant differences were also expected due to the low sample size and high variation. According to another study, the increasing levels of ALT and AST were associated with tumor progression (
26, 27).
The malignant group had 2.5-fold significantly higher value of AP compared to the benign group. MNL had significantly higher value than ML. The higher concentration in the malignant groups was expected due to the enzyme’s non-specific nature regarding pathological conditions and its high prevalence in different tissues, including the spleen. It could be considered as an indirect biomarker of intensive mitotic division in the spleen or with increased metastatic potential of hepatic or hepatobiliary malignant cells. Metabolic stress syndrome with endogenous cortisol level can induce elevated AP levels (
25, 28).
The limitations of the study are the low sample size in the groups which yielded low statistical power of 0.20 (20%). Therefore, the findings could be considered as merely indicative and could be used for further research by increasing the sample size.
CONCLUSIONThe ultrasonographic finding of heterogenous hypoechoic nodules with ‘leopard’ pattern morphology of the spleen, and pleomorphic lymphoblasts infiltration with increased values of leucocytes, neutrophils, monocytes, alanine transaminase, and alkaline phosphatase, are clear indicators for distinguishing malignant from benign NSD in dogs. The ultrasonographic and cytology findings, combined with higher values of leucocytes, neutrophils, and alkaline phosphatase, can be used for distinguishing lymphoid from non lymphoid NSD in dogs. None of these parameters alone could be used as a direct diagnostic indicator for NSD.
CONFLICT OF INTERESTThe authors declare that they have no financial or non-financial conflict of interest regarding authorship and publication of this article.
ACKNOWLEDGMENTSThe study was conducted on admitted patients at the University Veterinary Hospital at the Faculty of Veterinary Medicine-Skopje, together with colleagues from private practice.
AUTHORS’ CONTRIBUTIONIC performed the hematology, biochemistry, and cytology analyses and wrote the manuscript. AA collected and analyzed the data. IU revised the written text. EAP and TN performed the ultrasonographic diagnostics. MN conducted a detailed statistical analysis and made corrections to the final version of the manuscript.

 10.2478/macvetrev-2026-0017
10.2478/macvetrev-2026-0017